A nurse is caring for four clients for whom she has to administer oral medications in the morning. The nurse should administer which of the following medications before breakfast?
Levothyroxine
Digoxin
Divalproex
Mycostatin mouthwash
The Correct Answer is A
A. Levothyroxine
Correct Answer: Levothyroxine should be administered before breakfast.
Explanation: Levothyroxine is a synthetic thyroid hormone used to treat hypothyroidism. It needs to be taken on an empty stomach, at least 30 minutes before eating, to ensure proper absorption. Food can interfere with its absorption, especially foods containing calcium, iron, and fiber.
B. Digoxin
Incorrect Explanation: Digoxin does not need to be administered before breakfast.
Explanation: Digoxin is a medication used to treat heart conditions like congestive heart failure and atrial fibrillation. It doesn't have specific instructions regarding administration in relation to meals. It's important to administer digoxin consistently at the same time every day, but it doesn't need to be taken specifically before or after breakfast.
C. Divalproex
Incorrect Explanation: Divalproex does not need to be administered before breakfast.
Explanation: Divalproex is used to treat conditions like epilepsy and bipolar disorder. It can be taken with or without food. While taking it with food might reduce the likelihood of stomach upset, there's no requirement to take it specifically before breakfast.
D. Mycostatin Mouthwash
Incorrect Explanation: Mycostatin mouthwash is not related to breakfast timing.
Explanation: Mycostatin is an antifungal medication used to treat fungal infections in the mouth (oral thrush). Its administration is not linked to meal times. It's typically swished around in the mouth and then swallowed or spit out, depending on the specific instructions provided by the healthcare provider.

Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
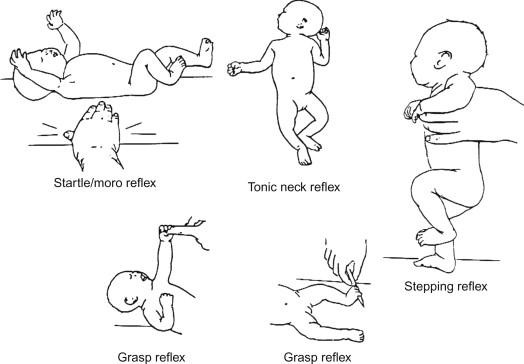
Reflexes play a crucial role in evaluating the neurological status of infants.
Moro reflex: Also known as the startle reflex, the Moro reflex is a normal response in infants. It occurs when an infant is startled by a sudden noise or movement. The baby responds by extending their arms and legs, followed by a quick contraction. This reflex usually disappears around 4-6 months of age.
Tonic neck reflex (fencer's reflex): This reflex involves turning an infant's head to one side, causing the arm on that side to extend and the opposite arm to flex. It's a normal reflex that typically disappears around 4-6 months of age.
Withdrawal reflex: The withdrawal reflex is a normal response to a stimulus, such as touching a baby's foot with a cold object. The baby will pull their leg away in response to the stimulus.
Symptomatic of decorticate or decerebrate posturing (options A and B):
Decorticate and decerebrate posturing are abnormal postures seen in individuals with severe brain damage or injury. Decorticate posturing involves the arms being flexed and held close to the body, while decerebrate posturing involves the arms being extended and the wrists being pronated. These reflexes are typically indicative of significant neurological dysfunction and are not expected in a 2-month-old infant after a car accident.
Indicators of severe brain damage (option C):
The reflexes described (Moro, tonic neck, and withdrawal reflexes) are not indicative of severe brain damage in a 2-month-old infant. These reflexes are normal for an infant of this age and are part of their typical neurological development.
Normal findings (option D):
The reflexes described are normal findings in a 2-month-old infant and are expected as part of their developmental milestones.
Correct Answer is D
Explanation
A. Polyuria (excessive urination) is not a symptom of hypoglycemia; it is more commonly associated with hyperglycemia (high blood sugar).
B. Deep rapid respirations are more characteristic of diabetic ketoacidosis (DKA), a complication of uncontrolled diabetes that leads to high blood sugar levels and metabolic acidosis.
C. Dry, flushed skin is not a typical symptom of hypoglycemia; it might be associated with conditions like dehydration or heat exposure, but not with low blood sugar.
D. Tachycardia
Explanation: The symptoms described by the adolescent (feeling shaky, difficulty speaking, difficulty concentrating) along with a blood glucose level of 55 mg/dL indicate hypoglycemia, which is low blood sugar. Tachycardia, or a rapid heart rate, is a common physiological response to hypoglycemia. The body increases the heart rate in an attempt to improve blood flow and deliver glucose to the brain and other vital organs. This is part of the body's fight-or-flight response to low blood sugar.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today