A nurse is caring for an older adult client who has a prescription for lorazepam 0.5 mg. Which of the following findings should the nurse report to the provider immediately?
Disorientation
Anorexia
Increased anxiety
Blurred vision
The Correct Answer is A
A. Disorientation in an older adult after taking lorazepam could indicate an adverse reaction or an excessive sedative effect. It's crucial to report this immediately as it may signify an overdose or an adverse reaction to the medication. Older adults are more sensitive to the sedative effects of benzodiazepines, and disorientation can indicate potential serious side effects.
B. Anorexia (loss of appetite) is a possible side effect of lorazepam but is not typically considered an urgent or immediate concern unless it leads to severe dehydration or other complications.
C. Increased anxiety could potentially occur due to paradoxical reactions to benzodiazepines; however, it's not typically considered an urgent or immediate concern unless it's severe or distressing to the client.
D. Blurred vision is a common side effect of lorazepam and other benzodiazepines. While it should be monitored and reported, it might not be considered an urgent concern unless it's significantly affecting the client's ability to function or is accompanied by other severe symptoms.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
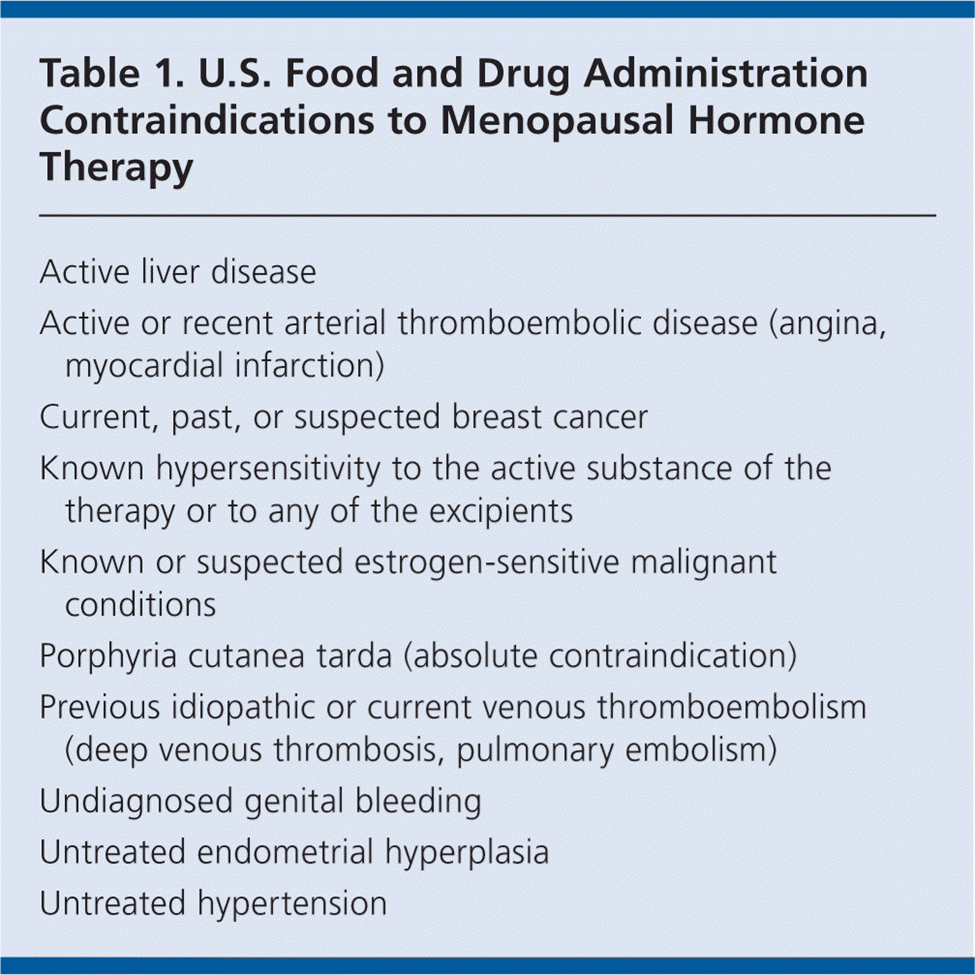
A. Concurrent treatment for GERD (gastroesophageal reflux disease) is not typically a contraindication for hormone replacement therapy. However, it's essential to assess the specific details of the client's medical history and medications to ensure safe use.
B. A history of breast cancer is a significant contraindication for hormone replacement therapy. Estrogen, a component of many HRT regimens, can stimulate the growth of certain types of breast cancer. Therefore, HRT is generally avoided in individuals with a history of breast cancer.
C. A history of dermatitis is not typically a contraindication for hormone replacement therapy. However, individual circumstances should be considered, and any concerns related to skin conditions should be discussed with the healthcare provider.
D. Multiple hospitalizations for COPD (chronic obstructive pulmonary disease) may not be a direct contraindication for hormone replacement therapy, but the overall health status and individual medical history should be carefully considered before initiating HRT.
Correct Answer is ["D","E"]
Explanation
A. Place the child in prone position:
Placing the child in a prone position (lying face down) during a seizure can obstruct the airway and lead to potential breathing difficulties.
B. Restrain the child:
Restraining a child during a seizure can cause injury or increase agitation. It's important to allow the child to move safely and avoid trying to hold them down.
C. Place a tongue depressor in the child's mouth:
It is not recommended to place anything, including a tongue depressor, in the child's mouth during a seizure. Doing so can cause injury to the child's teeth or oral structures.
D. Clear the area of hard objects:
Removing hard or sharp objects from the vicinity helps prevent injury to the child during the seizure.
E. Loosen restrictive clothing:
Loosening any tight clothing, especially around the neck, chest, or waist, allows the child to breathe more easily and reduces potential constriction during the seizure.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today