A nurse is caring for an adolescent who lives on their own and is refusing treatment. Which of the following statements should the nurse make? You can only refuse treatment for STI testing.
You will need a parent or guardian to make this medical decision for you.
You must be married in order to make your own health care decisions.
You have the right to refuse this treatment.
The Correct Answer is D
Choice A reason:
The nurse should inform the adolescent of their right to refuse treatment because respecting the patient's autonomy and right to make their own decisions about their healthcare is essential. This is especially true for an adolescent who is living on their own, as they have the legal capacity to make their medical decisions independently.
Choice B reason:
This statement is incorrect because, in most jurisdictions, adolescents who live on their own are considered emancipated minors, meaning they have the legal right to make their medical decisions without involving a parent or guardian. Requiring a parent or guardian's consent would not be applicable in this situation.
Choice C reason:
This statement is incorrect and irrelevant to the situation. Marriage status does not determine an individual's ability to make their own health care decisions. Regardless of marital status, an adolescent living on their own has the right to make their medical choices.
Choice D reason:
This is the correct choice. The nurse should emphasize the adolescent's right to refuse treatment if they wish to do so. It is crucial to respect their autonomy and ensure that they are fully informed about the potential consequences of their decision. However, the nurse should also provide relevant information about the treatment's benefits and risks to help the patient make an informed decision.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason:
Airborne precautions are implemented for diseases that spread through small airborne particles, such as tuberculosis or measles. These diseases can remain suspended in the air for extended periods and be inhaled by others. Pertussis, also known as whooping cough, is primarily spread through respiratory droplets when an infected person coughs or sneezes, making airborne precautions unnecessary.
Choice B reason:
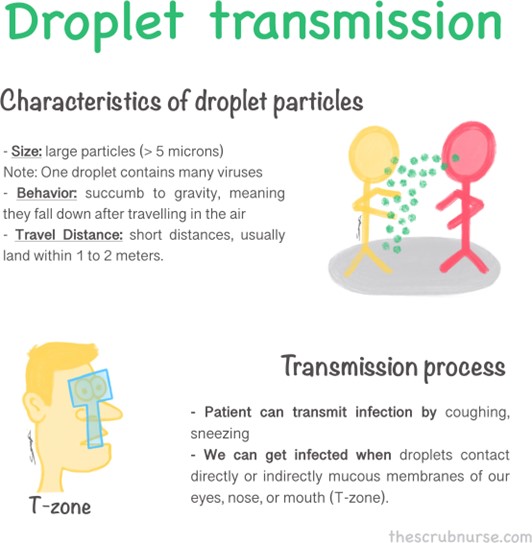
Droplet precautions are appropriate for illnesses that spread through respiratory droplets produced when an infected person talks, coughs, or sneezes. Pertussis falls into this category as it is transmitted mainly through respiratory droplets. By implementing droplet precautions, the nurse will minimize the risk of transmission to others, including healthcare workers and other patients.
Choice C reason:
Standard precautions are the baseline infection prevention practices used for all patients to prevent the spread of infections in healthcare settings. While important, they may not be sufficient to control the transmission of pertussis, as it requires additional measures like droplet precautions due to its specific mode of transmission.
Choice D reason:
Neutropenic precautions are used for patients with compromised immune systems, particularly those with low white blood cell counts (neutropenia). The purpose is to protect these vulnerable individuals from exposure to infectious agents. However, pertussis precautions are different and do not fall under the neutropenic category.
Correct Answer is D
Explanation
Choice A reason:
The client stating, "This test is to check if my baby has diabetes,” indicates a misunderstanding of the purpose of the 1-hr glucose tolerance test (GTT). The test is performed to screen for gestational diabetes in the mother, not to check the baby's diabetes status. Rationale: Gestational diabetes is a condition where high blood sugar levels develop during pregnancy, and it can affect both the mother and the baby's health.
Choice B reason:
The client mentioning, "If the result is higher than normal, I will need to be on insulin the rest of my life,” demonstrates a misconception about the implications of the 1-hr GTT. The 1-hr GTT is a preliminary screening test, and if the results are higher than normal, it indicates the need for further evaluation, but it does not immediately mean a lifetime dependence on insulin. Rationale: Insulin therapy may be required for managing gestational diabetes in some cases, but not necessarily for the rest of the mother's life.
Choice C reason:
The client saying, "If I forget and eat before the test, then I won't be able to have the test done,” indicates a misunderstanding of the test procedure. The 1-hr GTT requires fasting before the test, typically for 8 to 14 hours, to get accurate results. However, if the client mistakenly eats before the test, it doesn't mean they cannot have the test done at all; they may need to reschedule it after an appropriate fasting period. Rationale: Fasting is crucial for accurate glucose level measurement during the test.
Choice D reason:
The client stating, "If the results are high, then I need another test to see if I have gestational diabetes,” demonstrates a correct understanding of the 1-hr GTT. If the initial screening test shows elevated glucose levels, further testing, such as the 3-hour glucose tolerance test (GTT), is required to confirm the diagnosis of gestational diabetes. Rationale: The 3-hour GTT is a more comprehensive diagnostic test used to confirm or rule out gestational diabetes.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today