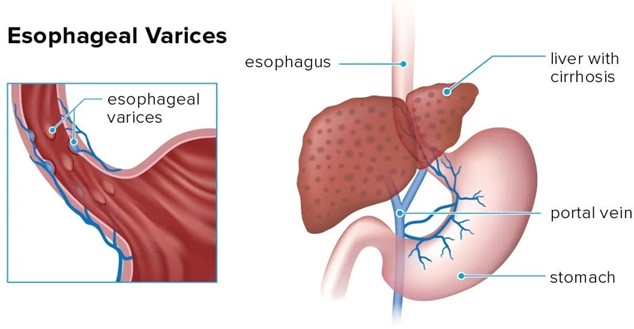
A nurse is caring for a client who was admited with bleeding esophageal varices and has an esophagogastric balloon tamponade with a Sengstaken-Blakemore tube to control the bleeding. Which of the following actions should the nurse take?
Provide frequent oral and nares care
Keep the client in a supine position
Ambulate the client four times per day
Encourage the client to consume clear liquids
The Correct Answer is A
Choice A: Provide frequent oral and nares care is the correct action for the nurse to take. Oral and nares care can help prevent infection, dryness, and irritation of the mucous membranes, which can be damaged by the pressure and friction of the tube. The nurse should also monitor the tube position, secure it with tape, and keep scissors at the bedside in case of emergency deflation.
Choice B: Keep the client in a supine position is not the correct action for the nurse to take. The supine position can increase the risk of aspiration, regurgitation, and gastric distension, which can worsen the bleeding and compromise the airway. The nurse should elevate the head of the bed to at least 30 degrees and use a semi-Fowler's or high-Fowler's position.
Choice C: Ambulating the client four times per day is not the correct action for the nurse to take. Ambulation can increase abdominal pressure and dislodge the tube, which can cause bleeding and perforation. The nurse should keep the client on bed rest and use passive range-of-motion exercises to prevent complications such as thromboembolism and muscle atrophy.
Choice D: Encouraging the client to consume clear liquids is not the correct action for the nurse to take. Clear liquids can increase gastric volume and acidity, which can aggravate the bleeding and interfere with hemostasis. The nurse should maintain a nothing-by-mouth status and provide intravenous fluids and nutrition as prescribed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason: This is incorrect because shortening of P-wave duration is not a sign of hyperkalemia or its reversal.
P-wave duration reflects the time it takes for the atria to depolarize and contract.
Choice B Reason: This is incorrect because restoration of QRS complex amplitude is not a sign of hyperkalemia or its reversal. QRS complex amplitude reflects the voltage or strength of the ventricular depolarization and contraction.
Choice C Reason: This is correct because the reduction of T-wave amplitude is a sign of hyperkalemia reversal. T-wave amplitude reflects the repolarization or recovery of the ventricles after contraction. Polystyrene sulfonate is a medication that lowers the serum potassium level by binding to it in the gastrointestinal tract and excreting it in the stool. High serum potassium level, or hyperkalemia, can cause cardiac arrhythmias and ECG changes, such as peaked T waves, prolonged PR interval, flatened P waves, widened QRS complex, and ventricular fibrillation. By lowering the serum potassium level, polystyrene sulfonate can reverse these ECG changes and normalize the cardiac rhythm.
Choice D Reason: This is incorrect because the widening of the QRS complex is a sign of hyperkalemia, not its reversal. Widening of the QRS complex reflects the delay or impairment of ventricular depolarization and contraction.

Correct Answer is D
Explanation
The correct answer is D. Blood pressure 115/68 mm Hg.
Choice A reason: Heart rate 180/min is incorrect because, although an increased heart rate is a compensatory mechanism, a rate of 180/min is excessively high and suggests a more severe stage of shock or other cardiac issues.
Choice B reason: Mottled skin is incorrect as it indicates poor perfusion seen in decompensated shock, where organ dysfunction begins to manifest, not in the compensatory stage.
Choice C reason: Hypokalemia, or low potassium levels, is incorrect because electrolyte imbalances are not typically a finding in the compensatory stage of shock. Normal potassium levels range from 3.5 to 5.0 mEq/L.
Choice D reason: Blood pressure 115/68 mm Hg is correct because it falls within the normal blood pressure range, which the body strives to maintain during the compensatory stage of shock through various mechanisms.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today