A nurse in an emergency department is caring for a client who is bleeding profusely from a deep laceration on his left lower forearm. After observing standard precautions, which of the following actions should the nurse perform first?
Clean the wound.
Apply a tourniquet just below the elbow.
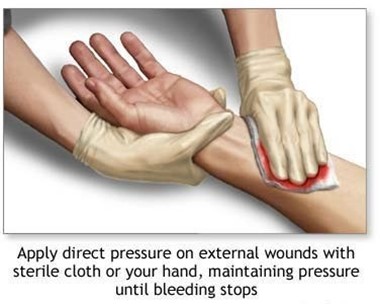
Apply direct pressure over the wound.
Elevate the limb and apply ice.
The Correct Answer is C
Choice A Reason: This is incorrect because cleaning the wound is not a priority when the client is bleeding profusely. Cleaning the wound can also dislodge any clots that have formed and increase bleeding.
Choice B Reason: This is incorrect because applying a tourniquet is a last resort when direct pressure fails to stop bleeding. A tourniquet can cause tissue damage, nerve injury, and infection if applied incorrectly or for too long.
Choice C Reason: This is correct because applying direct pressure over the wound is the first and most effective action to stop bleeding from a wound. This is the first and most effective action to stop bleeding from a wound. Direct pressure compresses the blood vessels and prevents further blood loss. The nurse should use a clean cloth or dressing to cover the wound and apply firm pressure with both hands.
Choice D Reason: This is incorrect because elevating the limb and applying ice are not effective actions to stop bleeding from a wound. Elevating the limb can reduce blood flow to the injured area, but it does not compress the blood vessels or prevent blood loss. Applying ice can cause vasoconstriction, but it can also damage the skin and tissues if applied for too long.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A: Cold and numb sensation distal to the fistula site is a possible indication of venous insufficiency. Venous insufficiency is a condition in which the veins have difficulty returning blood from the limbs to the heart, resulting in blood pooling and reduced perfusion. A new arteriovenous fistula can cause increased blood flow through the artery and decreased blood flow through the vein, leading to venous insufficiency. This can manifest as coldness, numbness, tingling, or cyanosis in the fingers or hand below the fistula site.
Choice B: A raised red rash around the fistula site is not a possible indication of venous insufficiency. A raised red rash around the fistula site can indicate an allergic reaction, an infection, or an inflammation of the skin or subcutaneous tissue. The nurse should assess the rash for size, shape, color, texture, temperature, and drainage, and report any signs of infection or inflammation, such as fever, pus, or swelling.
Choice C: Pain in the right arm proximal to the fistula site is not a possible indication of venous insufficiency. Pain in the right arm proximal to the fistula site can indicate arterial insufficiency, which is a condition in which the arteries have difficulty delivering oxygen-rich blood to the tissues, resulting in ischemia and necrosis. Arterial insufficiency can be caused by atherosclerosis, thrombosis, embolism, or vasospasm. The nurse should assess the pain for location, intensity, duration, frequency, and quality, and report any signs of ischemia or necrosis, such as pallor, coolness, weak pulses, or ulceration.
Choice D: Foul-smelling drainage from the fistula site is not a possible indication of venous insufficiency. Foul-smelling drainage from the fistula site can indicate an infection of the fistula or surrounding tissue. The nurse should assess the drainage for color, odor, amount, and consistency, and report any signs of infection or sepsis, such as fever, chills, malaise, or hypotension.
Correct Answer is C
Explanation
Choice A Reason: This is incorrect because droplet precautions are not sufficient to prevent the transmission of pneumonic plague. Droplet precautions are used to prevent the spread of infectious agents that are expelled through coughing, sneezing, or talking and travel only a short distance in the air. Droplet precautions include wearing a surgical mask, gown, and gloves, and placing the client in a private room or with a roommate who has the same infection.
Choice B Reason: This is incorrect because administering an antitoxin is not an intervention for pneumonic plague. An antitoxin is a substance that neutralizes the effects of a toxin produced by a microorganism. Pneumonic plague is not caused by a toxin, but by a bacterial infection.
Choice C Reason: This is correct because initiating airborne precautions is an intervention for pneumonic plague. Airborne precautions are used to prevent the spread of infectious agents that can remain suspended in the air and travel over long distances. Pneumonic plague is a severe and potentially fatal infection caused by the bacterium Yersinia pestis, which can be transmited through respiratory droplets or aerosols. Airborne precautions are used to prevent the spread of infectious agents that can remain suspended in the air and travel over long distances. Airborne precautions include wearing a respirator or N95 mask, placing the client in a negative-pressure room with an air filtration system, and limiting visitors and staff contact.
Choice D Reason: This is incorrect because destroying the linens after use is not an intervention for pneumonic plague. Linens that are contaminated with body fluids or secretions should be handled with gloves and placed in leak-proof bags for laundering or disposal, but they do not need to be destroyed.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today