A nurse is caring for a client who is scheduled to undergo thoracentesis. In which of the following positions should the nurse place the client for the procedure?
Prone with arms raised over the head.
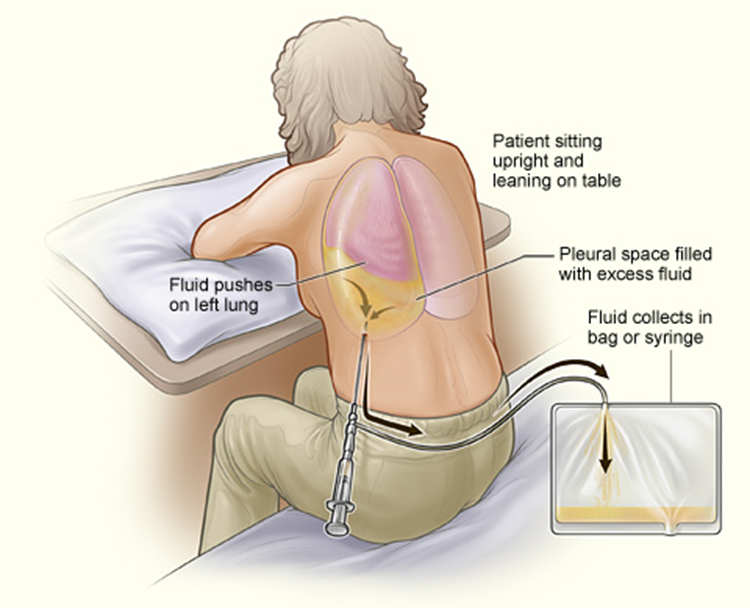
Sitting, leaning forward over the bedside table.
High Fowler's position
Side-lying with knees drawn up to the chest.
The Correct Answer is B
A. Prone with arms raised over the head.
This position involves lying face down with the arms raised over the head. It is not appropriate for thoracentesis because it does not provide easy access to the thoracic cavity, and it may compress the chest, making it difficult for the client to breathe comfortably during the procedure.
B. Sitting, leaning forward over the bedside table.
This is the correct choice. For thoracentesis, the client should be positioned sitting upright and leaning forward over the bedside table or supported by pillows. This position allows better access to the thoracic cavity and facilitates the removal of pleural fluid. Leaning forward also helps to open up the intercostal spaces, making it easier for the healthcare provider to insert the needle into the appropriate space between the ribs.
C. High Fowler's position.
The High Fowler's position involves the client sitting upright with the head of the bed elevated at a 90-degree angle. While this position may be used for other respiratory procedures or for comfort, it is not the optimal position for thoracentesis. It does not provide the same degree of access to the thoracic cavity as the sitting position with forward leaning.
D. Side-lying with knees drawn up to the chest.
This position involves lying on one side with the knees drawn up to the chest. It is not appropriate for thoracentesis because it does not provide access to the thoracic cavity, and it may obstruct the procedure. Additionally, this position may not be comfortable for the client during the procedure.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
First, we need to find out how many milligrams (mg) are in 1 milliliter (mL) of the available diphenhydramine solution:
12.5 mg/5 mL
To find out how many milligrams are in 1 mL, we divide the total milligrams by the total milliliters:
12.5 mg ÷ 5 mL = 2.5 mg/mL
Now that we know the concentration of diphenhydramine is 2.5 mg/mL, we can calculate the dose needed for the order of 25 mg:
25 mg ÷ 2.5 mg/mL = 10 mL
Correct Answer is C
Explanation
A. Constipation
Constipation is not typically associated with obstructive sleep apnea. However, sleep disturbances and certain medications used to manage OSA may indirectly contribute to constipation in some cases.
B. Nausea
Nausea is not a common symptom of obstructive sleep apnea. While sleep disturbances may affect gastrointestinal function in some individuals, nausea is not a typical manifestation of OSA.
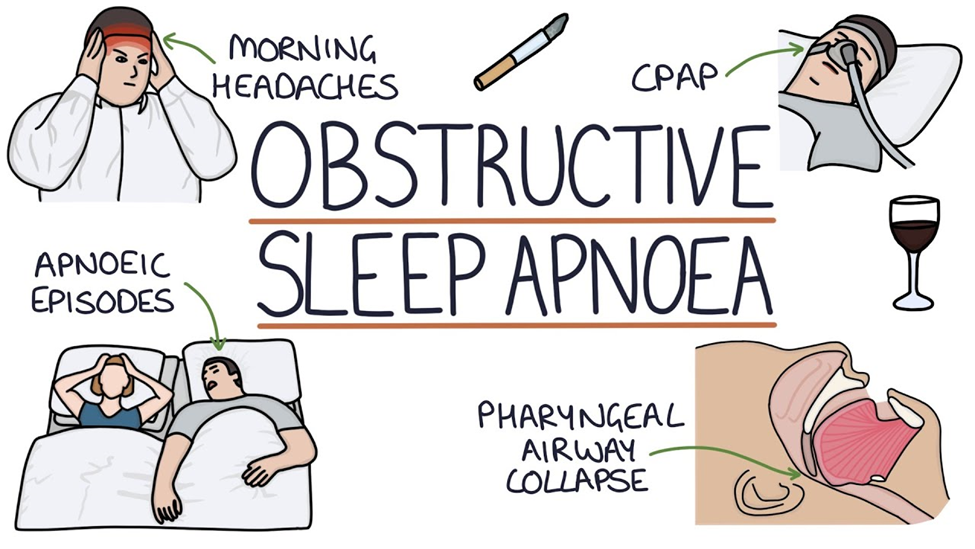
C. Headache
One of the common findings associated with obstructive sleep apnea (OSA) is headache. This occurs due to the repeated episodes of apnea (cessation of breathing) during sleep, which leads to intermittent hypoxia (low oxygen levels) and subsequent cerebral vasodilation. The vasodilation can trigger headaches, often described as morning headaches, upon waking up. These headaches are typically frontal and may be accompanied by other symptoms such as fatigue and irritability.
D. Hypotension
Hypotension (low blood pressure) is not a typical finding in obstructive sleep apnea. In fact, individuals with OSA are more likely to have hypertension (high blood pressure) due to the effects of repeated apnea episodes on the cardiovascular system, such as increased sympathetic activity and arterial stiffness.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today