A nurse is caring for a client who has developed a Clostridium difficile infection following antibiotic therapy. Which of the following actions should the nurse take?
Implement neutropenia isolation.
Use alcohol hand sanitizer following client care.
Monitor the client for manifestations of fluid overload.
Disinfect equipment with bleach solution
The Correct Answer is D
Choice A: Implement neutropenia isolation. This is not an action that the nurse should take for a client who has developed a Clostridium difficile infection. Neutropenia isolation is a type of protective isolation that is used for
clients who have low white blood cell counts and are at risk of infection from others. It is not indicated for clients who have Clostridium difficile infection, which is not transmited through the air.
Choice B: Use alcohol hand sanitizer following client care. This is not an action that the nurse should take for a client who has developed a Clostridium difficile infection. Alcohol hand sanitizer is ineffective against Clostridium difficile spores and can increase the risk of transmission. The nurse should wash their hands with soap and water, which can remove the spores from the skin.
Choice C: Monitor the client for manifestations of fluid overload. This is not an action that the nurse should take for a client who has developed a Clostridium difficile infection. Fluid overload is a condition that occurs when the body retains excess fluid and causes symptoms such as edema, dyspnea, and hypertension. It is not related to Clostridium difficile infection, which can cause fluid loss due to diarrhea and dehydration. The nurse should monitor the client for manifestations of fluid deficit, such as dry mucous membranes, tachycardia, and hypotension.
Choice D: Disinfect equipment with bleach solution. This is an action that the nurse should take for a client who has developed a Clostridium difficile infection, which is a bacterial infection that causes severe diarrhea and inflammation of the colon. Clostridium difficile spores are resistant to most disinfectants and can survive on surfaces for a long time. The nurse should disinfect equipment with bleach solution, which can kill the spores and prevent transmission.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A: Weak pulse. This is not a manifestation that the nurse should expect to find in a client who has advanced cirrhosis. A weak pulse may indicate hypovolemia, shock, or cardiac dysfunction, but it is not directly related to liver disease.
Choice B: Dark colored stools. This is not a manifestation that the nurse should expect to find in a client who has advanced cirrhosis. Dark colored stools may indicate bleeding in the upper gastrointestinal tract, such as from esophageal varices or peptic ulcers, but they are not specific to liver disease.
Choice C: Spider angioma. This is a manifestation that the nurse should expect to find in a client who has advanced cirrhosis, which is a chronic liver disease that causes scarring and impaired liver function. Spider angioma is a type of vascular lesion that appears as a red spot with radiating branches on the skin, usually on the face, neck, chest, or upper arms. It is caused by increased estrogen levels due to reduced liver metabolism of hormones.
Choice D: Increased body hair. This is not a manifestation that the nurse should expect to find in a client who has advanced cirrhosis. Increased body hair may indicate hypertrichosis, which is excessive hair growth due to genetic, hormonal, or metabolic factors, but it is not related to liver disease.
Correct Answer is B
Explanation
Choice A: Upper left quadrant. This is not the location where the nurse should expect the client to report abdominal pain who has diverticular disease. The upper left quadrant of the abdomen contains organs such as the stomach, spleen, pancreas, and part of the colon. Abdominal pain in this area can indicate conditions such as gastritis, peptic ulcer, pancreatitis, splenomegaly, or colon cancer.
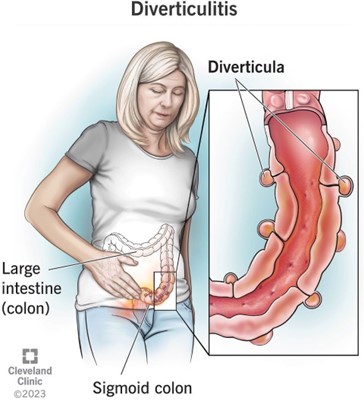
Choice B: Lower left quadrant. This is the location where the nurse should expect the client to report abdominal pain who has diverticular disease, which is a condition that involves the formation of pouches or sacs in the wall of the colon. These pouches or sacs are called diverticula, and they can become inflamed or infected, causing diverticulitis. Diverticulitis can cause abdominal pain, fever, nausea, vomiting, and changes in bowel habits. The most common site of diverticula formation and diverticulitis is the sigmoid colon, which is located in the lower left quadrant of the abdomen.
Choice C: Upper right quadrant. This is not the location where the nurse should expect the client to report abdominal pain who has diverticular disease. The upper right quadrant of the abdomen contains organs such as the liver, gallbladder, duodenum, and part of the colon. Abdominal pain in this area can indicate conditions such as hepatitis, cholecystitis, duodenal ulcer, or colon cancer.
Choice D: Lower right quadrant. This is not the location where the nurse should expect the client to report abdominal pain who has diverticular disease. The lower right quadrant of the abdomen contains organs such as the appendix, cecum, and part of the colon. Abdominal pain in this area can indicate conditions such as appendicitis, Crohn’s disease, or colon cancer.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today