A nurse in a clinic is caring for a client who has a new diagnosis of hypothyroidism. Which of the following findings should the nurse expect?
Palpitations
Weight gain
Diaphoresis
Protruding eyeballs
The Correct Answer is B
Choice A: Palpitations. This is not a finding that the nurse should expect in a client who has a new diagnosis of hypothyroidism, but rather a sign of hyperthyroidism, which is a condition that occurs when the thyroid gland produces too much thyroid hormone. Hyperthyroidism can cause palpitations due to increased cardiac output and heart rate.
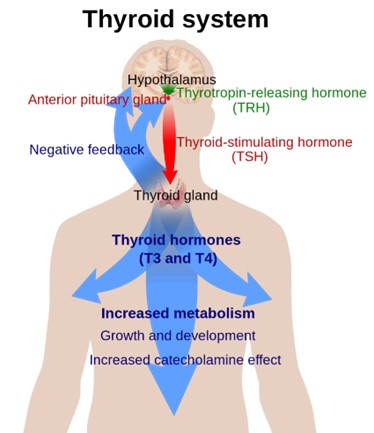
Choice B: Weight gain. This is a finding that the nurse should expect in a client who has a new diagnosis of hypothyroidism, which is a condition that occurs when the thyroid gland does not produce enough thyroid hormone. The thyroid hormone regulates the metabolism of carbohydrates, proteins, and fats, and affects energy expenditure and body temperature. Hypothyroidism can cause weight gain due to decreased metabolic rate and increased fluid retention.
Choice C: Diaphoresis. This is not a finding that the nurse should expect in a client who has a new diagnosis of hypothyroidism, but rather a sign of hyperthyroidism. Hyperthyroidism can cause diaphoresis due to increased heat production and vasodilation.
Choice D: Protruding eyeballs. This is not a finding that the nurse should expect in a client who has a new diagnosis of hypothyroidism, but rather a sign of Graves’ disease, which is an autoimmune disorder that causes hyperthyroidism. Graves’ disease can cause protruding eyeballs due to inflammation and edema of the orbital tissues and muscles.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A: Docusate. This is not a treatment that the nurse should expect to administer to a client with an acute exacerbation of ulcerative colitis. Docusate is a stool softener that can prevent constipation and straining, but it is not indicated for ulcerative colitis.
Choice B: A corticosteroid medication. This is a treatment that the nurse should expect to administer to a client with an acute exacerbation of ulcerative colitis, which is a chronic inflammatory bowel disease that causes ulcers and inflammation in the colon and rectum. A corticosteroid medication, such as prednisone, can reduce inflammation, suppress the immune system, and relieve symptoms such as diarrhea, bleeding, and pain.
Choice C: Aspirin. This is not a treatment that the nurse should expect to administer to a client with an acute exacerbation of ulcerative colitis. Aspirin is a nonsteroidal anti-inflammatory drug (NSAID) that can relieve pain and inflammation, but it can also irritate the gastrointestinal mucosa and worsen ulcerative colitis.
Choice D: A bowel cathartic medication. This is not a treatment that the nurse should expect to administer to a client with an acute exacerbation of ulcerative colitis. A bowel cathartic medication, such as bisacodyl, can stimulate bowel movements and cleanse the colon, but it can also cause dehydration, electrolyte imbalance, and aggravate ulcerative colitis.
Correct Answer is A
Explanation
Choice A: Sedentary lifestyle. This is a risk factor for developing type 2 diabetes mellitus, which is a condition that occurs when the body becomes resistant to the action of insulin or does not produce enough insulin to maintain normal blood glucose levels. Insulin is a hormone that helps glucose enter the cells and be used for energy. A sedentary lifestyle can increase the risk of type 2 diabetes mellitus by reducing physical activity, which can improve insulin sensitivity and lower blood glucose levels.
Choice B: Triglyceride level of 100 mg/dL. This is not a risk factor for developing type 2 diabetes mellitus, but rather a normal value. Triglycerides are a type of fat that circulates in the blood and can be used for energy or stored in adipose tissue. A high triglyceride level can indicate an increased risk of cardiovascular disease, but it is not directly related to type 2 diabetes mellitus.
Choice C: Blood glucose of 98 mg/dL. This is not a risk factor for developing type 2 diabetes mellitus, but rather a normal value. Blood glucose is the amount of glucose in the blood, which can vary depending on food intake, physical activity, and hormonal regulation. A high blood glucose level can indicate type 2 diabetes mellitus, but it is not a cause of it.
Choice D: Recent viral infection. This is not a risk factor for developing type 2 diabetes mellitus, but rather a possible trigger for type 1 diabetes mellitus, which is a condition that occurs when the immune system destroys the beta cells of the pancreas that produce insulin. A viral infection can trigger an autoimmune response that attacks the beta cells and causes type 1 diabetes mellitus.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today