A nurse is assisting with the care of a client who is 1 day postoperative following a thyroidectomy and reports severe muscle spasms of the lower extremities. Which of the following actions should the nurse take?
Determine the client’s calcium level.
Give the client an oral potassium supplement.
Administer intravenous normal saline solution.
Monitor the client’s peripheral pulses.
The Correct Answer is A
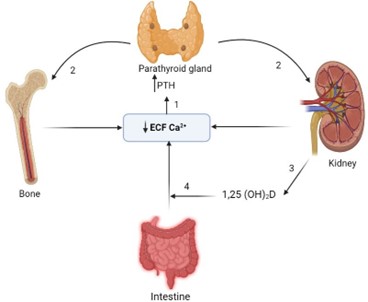
Choice A: Determine the client’s calcium level. This is the priority action for the nurse to take because the client might have hypocalcemia, which is a low level of calcium in the blood. Hypocalcemia can occur after a thyroidectomy due to accidental removal or damage of the parathyroid glands, which regulate calcium levels. Hypocalcemia can cause muscle spasms, tetany, paresthesia, and seizures.
Choice B: Give the client an oral potassium supplement. This is not an appropriate action for the nurse to take because the client might have hyperkalemia, which is a high level of potassium in the blood. Hyperkalemia can also occur after a thyroidectomy due to damage to the adrenal glands, which regulate potassium levels. Hyperkalemia can cause muscle weakness, arrhythmias, and cardiac arrest.
Choice C: Administer intravenous normal saline solution. This is not a necessary action for the nurse to take because the client does not have signs of dehydration or fluid imbalance. Normal saline solution does not affect calcium or potassium levels.
Choice D: Monitor the client’s peripheral pulses. This is an important action for the nurse to take, but not the priority. The nurse should monitor the client’s peripheral pulses for signs of decreased perfusion or ischemia, which can result from hypocalcemia or hyperkalemia affecting the cardiac function. However, this should be done after determining the client’s calcium level and correcting it if needed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A: Peri-umbilical area. This is not an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis. The peri-umbilical area is the area around the navel, which is part of the skin. The skin can show jaundice, but it may be difficult to detect in clients with dark skin tones.
Choice B: Nail beds. This is not an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis. The nail beds are part of the skin that can show jaundice, but they may also be affected by other factors such as anemia, cyanosis, or nail polish.
Choice C: Webbed areas of the fingers. This is not an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis. The webbed areas of the fingers are part of the skin that can show jaundice, but they may also be influenced by other factors such as temperature, circulation, or pressure.
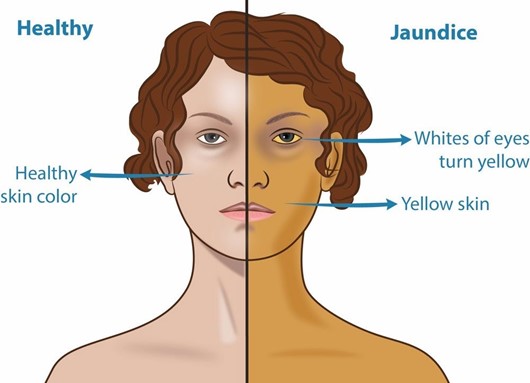
Choice D: Hard palate. This is an area that the nurse should inspect to monitor for the presence of jaundice in a client who is African American and has cholecystitis, which is an inflammation of the gallbladder. Jaundice is a yellowish discoloration of the skin and mucous membranes due to elevated bilirubin levels in the blood. Bilirubin is a pigment that is produced from the breakdown of red blood cells and is normally excreted in bile. If the gallbladder or bile ducts are inflamed or obstructed, bile cannot flow into the duodenum and bilirubin accumulates in the blood and tissues. The hard palate is a part of the oral mucosa that can show jaundice, especially in clients with dark skin tones.
Correct Answer is B
Explanation
Choice A: Increase the client’s sodium intake. This is not an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Increasing the client’s sodium intake can worsen fluid retention and exacerbate ascites. The nurse should recommend limiting the client’s sodium intake to less than 2 g per day.
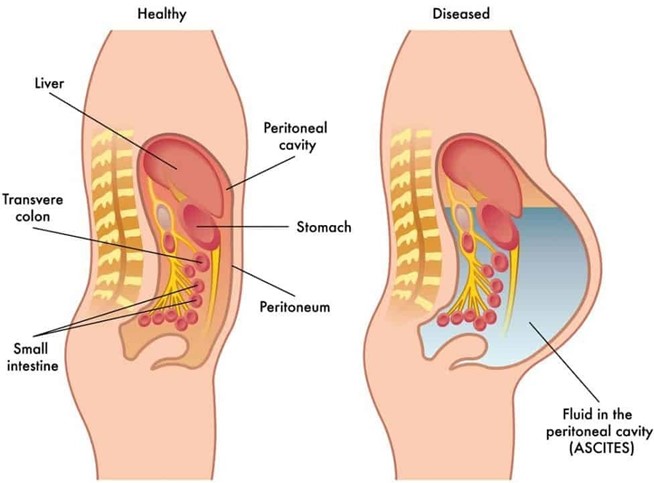
Choice B: Decrease the client’s fluid intake. This is an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Cirrhosis is a chronic liver disease that causes scarring and impaired liver function. Ascites is a complication of cirrhosis that involves the accumulation of fluid in the peritoneal cavity. Decreasing the client’s fluid intake can help reduce fluid retention and prevent further distension of the abdomen and pressure on the diaphragm.
Choice C: Increase the client’s saturated fat intake. This is not an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Increasing the client’s saturated fat intake can increase the risk of cardiovascular disease, obesity, and faty liver disease. The nurse should recommend a balanced diet that provides adequate protein, calories, vitamins, and minerals.
Choice D: Decrease the client’s carbohydrate intake. This is not an intervention that the nurse should recommend for inclusion in the plan of care for a client who has cirrhosis and ascites. Decreasing the client’s carbohydrate intake can cause ketosis, which is a metabolic state that occurs when the body uses fat as a fuel source instead of glucose.
Ketosis can cause nausea, fatigue, headache, and bad breath. The nurse should recommend a moderate carbohydrate intake that provides enough glucose for energy and prevents ketosis.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today