A nurse is caring for a client who has a new diagnosis of terminal cancer. Which of the following interventions is the priority?
Help the client to find a local support group.
Discuss the client's prior coping mechanisms.
Develop a list of goals with the client.
Teach the client to use progressive relaxation techniques.
Teach the client to use progressive relaxation techniques.
The Correct Answer is B
The priority intervention for a client with a new diagnosis of terminal cancer is to discuss the client's prior coping mechanisms. This will help the nurse to understand how the client has coped with difficult situations in the past and to develop a plan of care that is tailored to the client's individual needs and preferences.
Options a, c, and d are also important interventions, but they are not the priority. Helping the client to find a local support group, developing a list of goals with the client, and teaching the client to use progressive relaxation techniques can all be helpful in supporting the client's emotional well-being, but they should be implemented after the nurse has assessed the client's coping mechanisms and developed a plan of care.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
The priority intervention for a client with a new diagnosis of terminal cancer is to discuss the client's prior coping mechanisms. This will help the nurse to understand how the client has coped with difficult situations in the past and to develop a plan of care that is tailored to the client's individual needs and preferences.
Options a, c, and d are also important interventions, but they are not the priority. Helping the client to find a local support group, developing a list of goals with the client, and teaching the client to use progressive relaxation techniques can all be helpful in supporting the client's emotional well-being, but they should be implemented after the nurse has assessed the client's coping mechanisms and developed a plan of care.
Correct Answer is A
Explanation
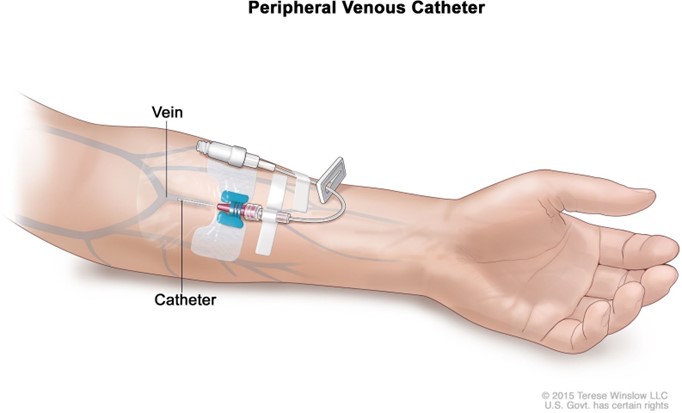
The correct answer is that the nurse should dangle the client's arm over the edge of the bed to help dilate the vein. This technique uses gravity to increase blood flow to the arm and dilate the veins, making it easier to insert a peripheral IV catheter.
Options b, c and d are not effective techniques for dilating a vein for IV insertion. Stroking the skin near the vein in an upward direction, instructing the client to flex their arm with the hand open and applying a cool compress to the vein for 10 min are not effective methods for dilating a vein.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today