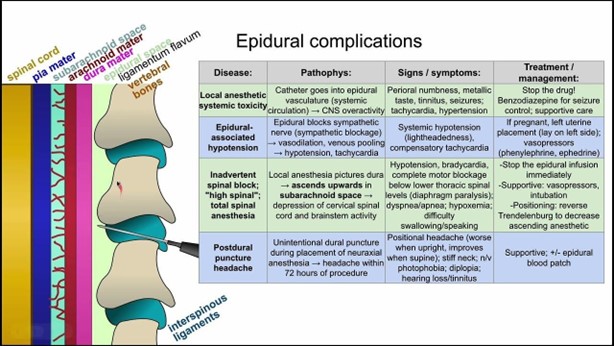
A nurse is assisting with the care of a client who is receiving a spinal epidural to treat a herniated disc.
Which of the following findings should the nurse identify as an indicator of unrelieved pain?
Urinary retention
Constipation
Difficulty swallowing
Restlessness
The Correct Answer is D
Restlessness can be an indicator of unrelieved pain in a client who is receiving a spinal epidural to treat a herniated disc. Restlessness is often a manifestation of discomfort or agitation, which can be caused by inadequate pain management. When a client's pain is not adequately relieved, they may exhibit restlessness as they try to find a more comfortable position or seek relief from the discomfort.
Urinary retention (option A) is incorrect because it can be a side effect of certain medications used in pain management, such as opioids, but it is not a specific indicator of unrelieved pain. It is important to monitor for urinary retention as a potential complication of spinal epidural anaesthesia, but it is not directly related to pain relief.
Constipation (option B) is incorrect because it is another possible side effect of opioid medications, but it is not a specific indicator of unrelieved pain. It is important to address constipation as a potential adverse effect of pain management, but it is not a direct indicator of pain relief.
Difficulty swallowing (option C) is incorrect because it is not a common indicator of unrelieved pain in the context of a spinal epidural. It may be associated with other conditions or complications but is not specifically related to pain relief.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
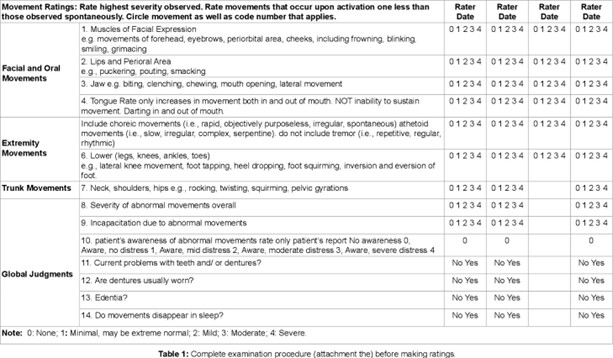
The AIMS is specifically designed to assess for the presence and severity of abnormal involuntary movements, which can be a side effect of long-term antipsychotic medication use, including tardive dyskinesia. It consists of a series of standardized movements and observations that assess different body regions for abnormal movements. The nurse can use this tool to monitor the client's movements and identify any signs of tardive dyskinesia.
A. Mental Status Examination (MSE): The MSE is a comprehensive assessment of a client's mental status, including their cognition, mood, and thought processes. While the MSE is an important tool in assessing overall mental health, it is not specific to tardive dyskinesia.
C. Patient Health Questionnaire-9 (PHQ-9): The PHQ-9 is a screening tool for depression that assesses the severity of depressive symptoms. While depression can be a comorbidity in individuals with schizophrenia, the PHQ-9 does not directly assess for tardive dyskinesia.
D. Brief Psychiatric Rating Scale (BPRS): The BPRS is a rating scale used to assess the severity of psychiatric symptoms in individuals with mental disorders. While it is useful in evaluating overall symptomatology in schizophrenia, it does not specifically target tardive dyskinesia.
Correct Answer is C
Explanation
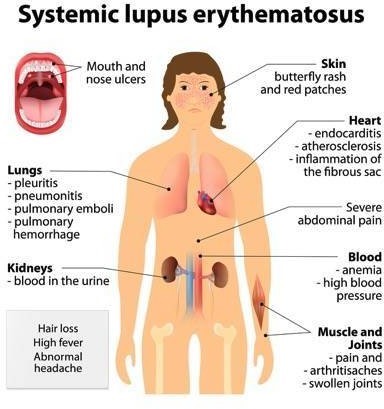
Systemic lupus erythematosus (SLE) is an autoimmune disease that can affect the skin. Proper skin care is important for individuals with SLE to minimize potential flare-ups or exacerbation of skin symptoms. The recommended approach to skin care in SLE includes gentle cleansing and moisturizing.
"I will use an astringent on my face." Astringents are typically not recommended for individuals with SLE as they can be harsh on the skin and may cause irritation or dryness.
"I will cleanse my skin using an antibacterial soap." While it is important to keep the skin clean, using an antibacterial soap is not specifically required for individuals with SLE. Gentle,
Non-irritating cleansers without antibacterial properties are generally recommended.
"I will limit my time in the tanning bed to 15 minutes." Exposure to ultraviolet (UV) radiation, such as from tanning beds, can be particularly harmful to individuals with SLE. UV radiation can trigger or worsen skin manifestations and may lead to disease flares. Therefore, it is generally advised for individuals with SLE to avoid tanning beds altogether.
In addition to gentle cleansing and moisturizing, individuals with SLE should also practice sun protection, including wearing sunscreen with a high sun protection factor (SPF) and using protective clothing and accessories (such as hats and sunglasses) when exposed to the sun. Regular check-ups with a healthcare provider and following their recommendations are important for managing SLE and its associated skin manifestations.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today