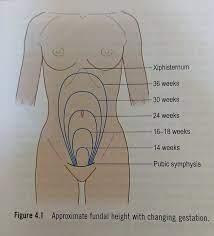
A nurse is assisting in obtaining the fundal height measurement for a client who is at 32 weeks of gestation. Which of the following images indicates where the nurse should expect the client's fundus to be located?
The fundal height corresponds with approximately 16 weeks.
The fundal height corresponds with approximately 20 weeks.
The fundal height corresponds with approximately 32 weeks.
The fundal height corresponds with approximately 24 weeks.
The Correct Answer is C
A) Incorrect- the fundal height corresponds with approximately 16 weeks. At around 16 weeks of gestation, the fundal height is usually located approximately at the midpoint between the symphysis pubis (pubic bone) and the belly button (umbilicus). This measurement corresponds to the anatomical level of the uterus at this stage.
B) Incorrect- the fundal height corresponds with approximately 20 weeks. By 20 weeks of gestation, the fundus has typically reached the level of the umbilicus. The fundal height measurement is around the same level as the belly button.
C) Correct- the fundal height corresponds with approximately 32 weeks. Around 32 weeks of gestation, the fundal height has increased significantly compared to earlier stages of pregnancy. The fundus of the uterus is located above the belly button, and the measurement is typically about 32 centimeters (or roughly 12.6 inches) above the symphysis pubis.
D) Incorrect- the fundal height corresponds with approximately 24 weeks. Around 24 weeks of gestation, the fundal height is usually about 1 to 2 fingerbreadths above the
umbilicus. This represents the ongoing upward growth of the uterus as the pregnancy progresses.
E) Incorrect- the fundal height corresponds with approximately 18 weeks. At around 18 weeks of pregnancy, the fundal height is typically located just above the pubic bone, below the belly button (umbilicus). The fundus of the uterus is still relatively low in the abdomen at this point. The fundal height measurement at 18 weeks is usually around the midpoint between the symphysis pubis (pubic bone) and the belly button.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A) Correct - Encouraging the client to void often is important, as a full bladder can increase discomfort and interfere with labor progress.
B) Incorrect- Remaining awake between contractions might not directly address pain management strategies.
C) Incorrect- Position changes can help with pain management, so minimizing them would not be appropriate.
D) Incorrect- The presence of a support person is often encouraged during labor, and there is no need to limit their time in the room.
Correct Answer is ["B","C","E"]
Explanation
A) Incorrect- Dry, cracked skin is not typically associated with a newborn born at 43 weeks of gestation. It's more common in post-term babies.
B) Correct - Hypotonia (low muscle tone) is a possible finding in post-term newborns due to the aging placenta and potential decrease in amniotic fluid.
C) Correct - Excessive lanugo (fine, downy hair) is more likely to be present in post-term babies as they have less vernix to protect their skin.
D) Incorrect- Absent vernix might be more characteristic of a post-term newborn, but its presence or absence varies widely.
E) Correct - Long, hard nails can be a characteristic of post-term babies, as they have had more time for nail growth in the womb.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today