A nurse is collecting data from a client who is receiving epidural anesthesia. Which of the following findings indicates an adverse effect of this method of pain management?
Tachycardia
Fever
Tachypnea
Hypertension
The Correct Answer is C
Rationale:
A. Tachycardia is not a common or direct adverse effect of epidural anesthesia itself. While a rapid heart rate may occur secondary to maternal anxiety or as a compensatory response to hypotension, it is not the primary physiological marker for epidural complications. Heart rate typically remains stable or may decrease slightly as pain is relieved and sympathetic activity is modulated.
B. Fever is a documented potential adverse effect associated with epidural anesthesia, particularly during labor. The exact mechanism is multifactorial, potentially involving altered thermoregulation, reduced heat dissipation due to sympathetic blockade, or a non-infectious inflammatory response. Clinicians must distinguish this pharmacological pyrexia from maternal infection to ensure appropriate neonatal and maternal management following the delivery.
C. Tachypnea, or an increased respiratory rate, is generally not associated with epidural anesthesia. In fact, if the anesthesia level rises too high, it can lead to respiratory depression or a decreased rate due to the blockade of intercostal muscle nerves. Effective epidural analgesia usually promotes a more relaxed, normal breathing pattern by successfully alleviating the physiological stress and hyperventilation caused by acute pain.
D. Hypertension is the opposite of the expected vascular response to epidural anesthesia. The local anesthetic typically causes a sympathetic blockade, leading to peripheral vasodilation and a significant risk of maternal hypotension rather than high blood pressure. Monitoring blood pressure is a critical nursing priority because decreased systemic vascular resistance can compromise placental perfusion and lead to fetal heart rate decelerations.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A) Correct- Feeling the baby's swallowing during breastfeeding indicates that the baby is effectively transferring milk from the breast. It suggests that the baby is latched on correctly and is receiving milk.
B) Incorrect- Moderate tenderness during breastfeeding is common initially, but it should not be persistent or severe.
C) Incorrect- While bowel movements are important, having at least one bowel movement every day is not necessarily an indicator of effective breastfeeding.
D) Incorrect- While wet diapers are important to ensure adequate hydration, having at least six wet diapers every day is not the primary sign of effective breastfeeding.
Correct Answer is C
Explanation
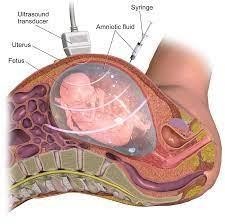
A) Incorrect- Leakage of fluid is possible but not a primary focus of post-procedure instructions.
B) Incorrect- Milk of magnesia is not relevant to an amniocentesis procedure.
C) Correct - Reporting uterine contractions after the procedure is important as it could indicate a potential complication, such as preterm labor.
D) Incorrect- Blood work drawn before the procedure is not typically part of the amniocentesis process.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today