A nurse is assessing pressure ulcers on four clients to evaluate the effectiveness of a change in wound care procedure. Which of the following findings indicates wound healing?
Increase in serosanguineous exudate from a client's wound
Deep red color on the center of a client's wound
Erythema on the skin surrounding a client's wound
Inflammation noted on the tissue edges of a client's wound
The Correct Answer is B
Choice A reason: This is not the correct choice because an increase in serosanguineous exudate (a mixture of blood and clear fluid) from a client's wound indicates infection, inflammation, or trauma to the wound. This is a sign of wound deterioration, not healing.
Choice B reason: This is the correct choice because a deep red color on the center of a client's wound indicates granulation tissue, which is new tissue that forms during the healing process. Granulation tissue fills the wound bed and provides a foundation for epithelialization (the growth of new skin over the wound).
Choice C reason: This is not the correct choice because erythema (redness) on the skin surrounding a client's wound indicates irritation, inflammation, or infection of the skin. This is a sign of wound complication, not healing.
Choice D reason: This is not the correct choice because inflammation on the tissue edges of a client's wound indicates infection, trauma, or necrosis (death) of the tissue. This is a sign of wound impairment, not healing.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason: The most recent blood glucose reading is not the most important information for the nurse to report at shift change. IV corticosteroids can cause hyperglycemia, which requires monitoring and treatment, but it is not as critical as the client's level of consciousness.
Choice B reason: The laboratory tests scheduled for next shift are not the most important information for the nurse to report at shift change. The nurse should inform the oncoming nurse about the tests, but they are not as urgent as the client's neurological status.
Choice C reason: The reddened area on the coccyx is not the most important information for the nurse to report at shift change. The nurse should document and report any signs of skin breakdown, but they are not as life-threatening as the client's increased intracranial pressure.
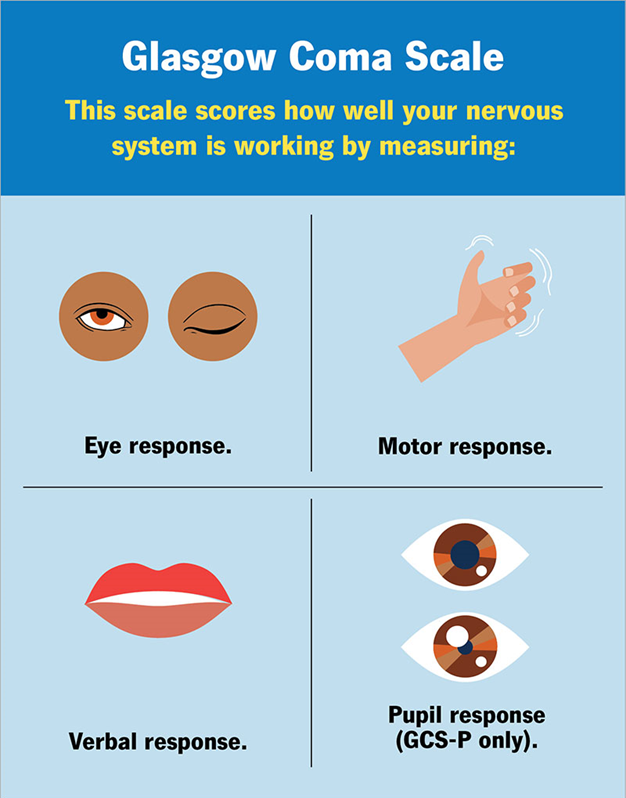
Choice D reason: The Glasgow Coma Scale score is the most important information for the nurse to report at shift change. The Glasgow Coma Scale is a tool that measures the client's level of consciousness based on eye opening, verbal response, and motor response. A decrease in the score indicates a deterioration in the client's neurological condition, which requires immediate intervention.
Correct Answer is C
Explanation
Choice A reason: This is not the correct choice because this response is insensitive and unprofessional. The nurse should not blame or criticize the client for signing the consent form, as this may make the client feel guilty or pressured. The nurse should respect the client's autonomy and right to change their mind.
Choice B reason: This is not the correct choice because this response is inadequate and irrelevant. The nurse should not assume that the client needs more information about the surgery, as this may not address the client's underlying reasons for being unsure. The nurse should listen to the client's concerns and provide emotional support.
Choice C reason: This is the correct choice because this response is respectful and reassuring. The nurse should acknowledge the client's feelings and let them know that they have the option to cancel the surgery if they are not comfortable with it. The nurse should also inform the provider and the surgical team about the client's situation and facilitate further discussion if needed.
Choice D reason: This is not the correct choice because this response is inappropriate and unethical. The nurse should not offer medication to the client to help them relax, as this may impair their decision-making capacity and consent. The nurse should not coerce or manipulate the client to undergo the surgery.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today