A nurse is assessing a client's peripheral circulation. In which of the following locations should the nurse palpate to assess the posterior tibial pulse? (Selectable areas, or "Hot Spots," are outlined in the artwork below. Select only the outlined area that corresponds to your answer.)
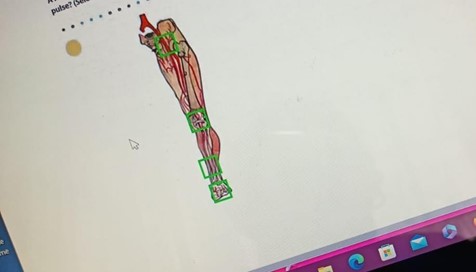
inguinal canal
knee
lower third of the tibia
dorsal aspect of the foot
The Correct Answer is C
A. Inguinal canal is not the correct location for assessing the posterior tibial pulse. This area is associated with the femoral pulse.
B. The knee is not the correct location for assessing the posterior tibial pulse. This area is not directly related to the posterior tibial pulse.
C. The lower third of the tibia, anterior aspect is the correct location for palpating the posterior tibial pulse. This pulse can be found on the inside of the ankle, slightly below and behind the medial malleolus.
D. Dorsal aspect of the foot is where the dorsalis pedis pulse is located, not the posterior tibial pulse.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
A. Measuring the gastric residual is a common practice before administering enteral feedings. It helps to assess if the client's stomach is emptying properly and if there is any buildup of undigested formula. This is important in identifying delayed gastric emptying, which can lead to complications if not addressed.
B. To remove gastric acid that might cause dyspepsia is not the primary purpose of measuring gastric residual. The main concern is to assess the rate of stomach emptying.
C. To confirm the placement of the NG tube is typically done using other methods, such as pH testing or an X-ray. While aspirating stomach contents through the tube can help confirm placement, it is not the primary purpose of measuring gastric residual.
D. To determine the client's electrolyte balance is not related to the purpose of measuring gastric residual. Electrolyte balance is typically assessed through blood tests and clinical signs and symptoms.
Correct Answer is D
Explanation
A. Irrigating the wound with an antiseptic prior to obtaining the specimen can introduce substances that may interfere with the accuracy of the culture results. Sterile saline is the preferred solution for wound irrigation.
B. Intact skin at the wound edges should not be included in the culture. The specimen should be obtained directly from the wound bed or drainage.
C. Swabbing an area of skin away from the wound to identify the usual flora is not appropriate for obtaining a wound drainage specimen. The culture should be taken directly from the wound site.
D. Before obtaining a wound-drainage specimen for culture, it is important to cleanse the wound with a sterile solution, such as 0.9% sodium chloride saline irrigation. This helps remove debris and contaminants from the wound site, providing a more accurate specimen for culture.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today