A nurse is assessing a client who is receiving penicillin IV.
For which of the following findings should the nurse report to the provider as a manifestation of anaphylaxis?
Hypertonia.
Wheezing.
Urinary retention.
Increased blood pressure.
The Correct Answer is B
Anaphylaxis is a severe, potentially life-threatening allergic reaction that can occur within seconds or minutes of exposure to an allergen, such as penicillin.
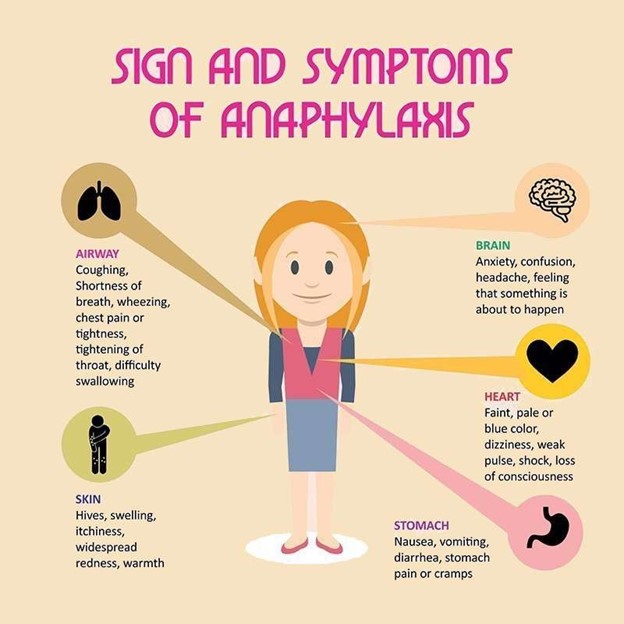
One of the symptoms of anaphylaxis is wheezing, which is caused by the constriction of the airways and a swollen tongue or throat.
Choice A is wrong because hypertonia (increased muscle tone) is not a known symptom of anaphylaxis.
Choice C is wrong because urinary retention (inability to completely empty the bladder) is not a known symptom of anaphylaxis.
Choice D is wrong because increased blood pressure is not a known symptom of anaphylaxis; in fact, anaphylaxis can cause a sudden drop in blood pressure.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
The nurse should instruct the client to monitor and report bruising as an adverse effect of taking clopidogrel.

Clopidogrel increases the risk of bleeding, which can be severe or life- threatening.
Choice A is wrong because blurred vision is not a common adverse effect of clopidogrel.
Choice B is wrong because constipation is not a common adverse effect of clopidogrel.
Choice C is wrong because weight loss is not a common adverse effect of clopidogrel.
Correct Answer is D
Explanation
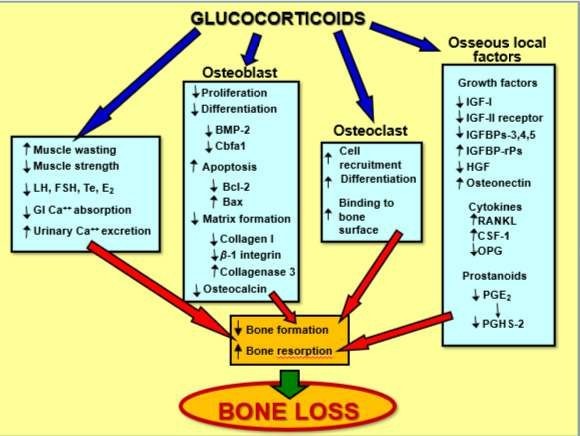
Prednisone is a corticosteroid that can be used to treat rheumatoid arthritis and other conditions by reducing inflammation and suppressing the immune system.
However, long-term use of prednisone can cause side effects, including bone loss.
Choice A is wrong because liver toxicity is not a common side effect of prednisone.
Choice B is wrong because hypoglycemia is not a common side effect of prednisone; instead, elevated blood sugar is a possible side effect.
Choice C is wrong because hemolytic anemia is not a common side effect of prednisone.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today