A nurse in the emergency department is assessing a newly admitted client who is experiencing drooling and hoarseness following a burn injury. Which of the following actions should the nurse take first?
Obtain a blood specimen for ABG analysis.
Apply 100% humidified oxygen.
Obtain a baseline ECG.
Insert an 18-gauge IV catheter.
The Correct Answer is B
A. Obtain a blood specimen for ABG analysis. Important, but not the first action.
B. In a client with burn injuries experiencing signs of airway compromise (drooling, hoarseness), the first action should be to ensure adequate oxygenation. Applying 100% humidified oxygen can help manage potential airway edema.
C. Obtain a baseline ECG. Necessary for monitoring but secondary to securing the airway.
D. Insert an 18-gauge IV catheter. Essential for fluid resuscitation and medication administration, but after ensuring adequate oxygenation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is {"dropdown-group-1":"C","dropdown-group-2":"C"}
Explanation
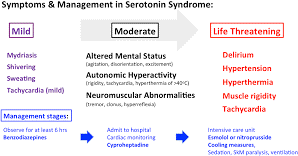
Serotonin syndrome is a serious drug reaction that results from having too much serotonin in the body. Serotonin is a chemical that plays a role in mood, sleep, appetite and other functions. Some medications, especially antidepressants, can increase serotonin levels and cause serotonin syndrome. The client is taking paroxetine, which is a type of antidepressant called a selective serotonin reuptake inhibitor (SSRI). SSRIs work by blocking the reabsorption of serotonin in the brain, making more serotonin available.
Paroxetine can cause serotonin syndrome if taken at high doses, in combination with
other serotonergic drugs, or if abruptly stopped. The client’s symptoms of restlessness, abdominal pain, disorientation and fever are consistent with serotonin syndrome. Other possible symptoms include agitation, confusion, rapid heart rate, high blood pressure, dilated pupils, muscle twitching, rigidity, sweating and shivering. Severe serotonin syndrome can lead to seizures, coma and death. The client should stop taking paroxetine and seek immediate medical attention. Serotonin syndrome can be treated with supportive care and medications that reduce serotonin levels or block its effects. The client may need to switch to a different antidepressant or adjust the dosage under the guidance of their provider.
Correct Answer is D
Explanation
A. This would involve irregular beats and potentially a visible compensatory pause, not a prolonged PR interval.
B. Atrial fibrillation features an irregularly irregular rhythm and no discernible PR intervals.
C. Defined by a heart rate less than 60/min with a normal rhythm and electrical pattern, which does not apply here given the normal rate and prolonged PR interval.
D. A first-degree atrioventricular (AV) block is characterized by a prolonged PR interval (greater than 0.20 seconds) in the presence of a normal heart rate and rhythm, which aligns with the client’s PR interval of 0.24 seconds and a heart rate of 69/min
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today