A nurse has just finished a wound irrigation for a client who requires contact precautions. Which of the following pieces of personal protective equipment (PPE) should the nurse remove first?
Gloves
Mask
Gown
Face shield
The Correct Answer is A
Choice A rationale: When removing personal protective equipment (PPE) after a procedure involving contact precautions, the nurse should remove the items in a specific order to minimize the risk of contamination. Gloves should be removed first because they are the most likely to be contaminated and can transfer microorganisms to other surfaces or PPE during removal.
Choice B rationale: The mask should be removed after gloves and gown. Removing the mask first could potentially contaminate the hands, leading to the risk of transferring microorganisms to the face during mask removal.
Choice C rationale: The gown should be removed after gloves and before the mask. Removing the gown too early could lead to potential contamination of the hands.
Choice D rationale: The face shield should be removed after gloves, mask, and gown. It provides additional protection for the face and should be retained until the end of the removal process to minimize the risk of contamination.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","C","D"]
Explanation
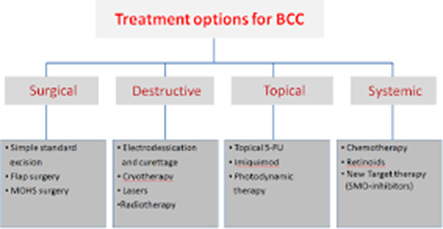
Choice A rationale: radiation therapy is one of the possible management options for basal cell carcinoma (BCC) that uses high-energy rays to kill the cancerous cells.
Choice B rationale: this is incorrect since topical corticosteroids are ineffective in BCC management and may worsen the patient’s condition by suppressing their immune system.
Choice C rationale: micrographic surgery can be used in BCC management and it involves the removal of thin layers of skin to a point where no cancer cells can be detected.
Choice D rationale: this is appropriate and involves the use of electric current to burn off the cancer cells.
Correct Answer is ["A","B","E"]
Explanation
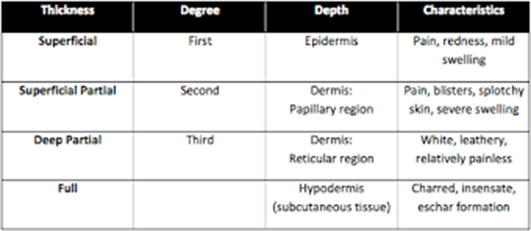
Choice A rationale: partial-thickness burns are usually characterized by the formation of blisters as a result of increased capillary permeability resulting in edema formation separating the epidermis from the dermis.
Choice B rationale: wound blanching with pressure is expected in partial-thickness burns due to compromised blood circulation.
Choice C rationale: This is not a typical finding in a partial-thickness burn.
Choice D rationale: this is incorrect since partial-thickness burns involve damage to the epidermis.
Choice E rationale: nerve endings are damaged in partial-thickness burns thus making the area sensitive to touch.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today