A nurse caring for a client who has depression observes the client comes to breakfast freshly bathed wearing clean clothes, and styled hair. Which of the following responses by the nurse is therapeutic?
"Why are you all dressed up today?”
“I see you have done some grooming today"
“Everyone feels better after showering”
"You must be getting better. You look great”
The Correct Answer is B
This response acknowledges the client's effort and self-care without making assumptions or imposing judgment. It is an open and non-intrusive statement that shows the nurse is paying attention to the client's appearance and recognizing their positive action of self-grooming. It allows the client to share their feelings or thoughts if they choose to without feeling pressured or judged. This response demonstrates empathy and understanding, creating a supportive and non-threatening environment for the client to express themselves if they wish to do so.
Incorrect:
A- "Why are you all dressed up today?" This question may put the client on the spot and make them feel self-conscious or defensive. It assumes that there must be a specific reason for the client's appearance, which may not be the case. It can also imply that the client's usual appearance is different or not as desirable.
C- "Everyone feels better after showering." While it is true that personal hygiene can have a positive impact on one's mood, this statement may come across as dismissive or oversimplifying the client's experience. It may invalidate any underlying emotions or struggles the client is facing with their depression. It is important to acknowledge and address the client's feelings rather than making broad generalizations.
D- "You must be getting better. You look great." This statement assumes that physical appearance is directly correlated with the client's mental health and suggests that improvement in appearance equates to improvement in mental well-being. However, a person's outward appearance may not accurately reflect their internal struggles or progress in managing depression. Additionally, it can create pressure for the client to maintain a certain appearance to be perceived as "better."
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
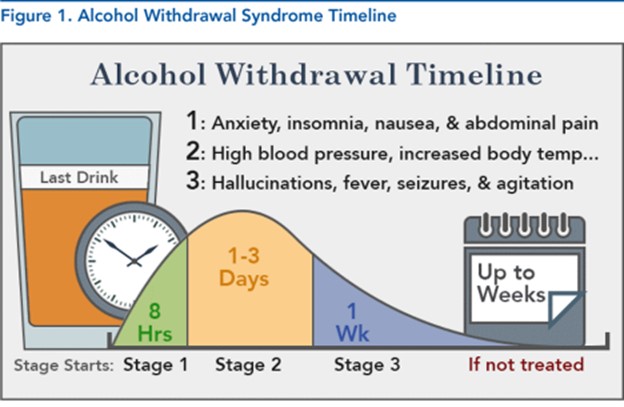
Anxiety and diaphoresis: Alcohol withdrawal commonly presents with symptoms of anxiety, restlessness, and excessive sweating (diaphoresis). These symptoms are due to the central nervous system's hyperactivity caused by the sudden cessation of alcohol intake.
Incorrect:
B- Muscle aches and chills: Muscle aches and chills are not typical manifestations of alcohol withdrawal. These symptoms are more commonly associated with opioid withdrawal rather than alcohol withdrawal.
C- Fatigue and depression: Fatigue and depression are common symptoms during alcohol withdrawal. The client may feel tired, lack energy, and experience a low mood due to the neurochemical imbalances that occur during withdrawal.
D- Arrhythmia and respiratory depression: While alcohol withdrawal can lead to some cardiovascular and respiratory symptoms, such as increased heart rate and blood pressure, severe arrhythmia and respiratory depression are not typical findings. These more severe symptoms may indicate a more severe withdrawal syndrome or coexisting medical conditions that require immediate medical attention.
Correct Answer is D
Explanation
This response demonstrates a therapeutic and empathetic approach to the client's distress. By offering to talk in a private area without interruption, the nurse provides the client with a safe space to express their feelings and concerns. It also allows the nurse to conduct a more in-depth assessment of the client's current emotional state and any specific triggers contributing to their anxiety.
A- Encouraging the client to lie down assumes that all clients with anxiety benefit from this approach, which may not be the case for everyone.
B- Simply suggesting medication may not address the underlying concerns or provide an opportunity for the client to express themselves.
C- While relaxation exercises can be beneficial for managing anxiety, suggesting them right away may not be the best response when the client is in a heightened state of distress.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today