A nurse accidentally administers the medication metformin instead of metoprolol to a client. Which of the following actions should the nurse take?
Check the client's glucose level.
Collect the client's uric acid level.
Obtain the client's HDL level.
Monitor the client's thyroid function levels.
The Correct Answer is A
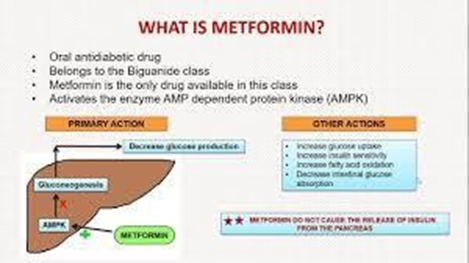
Choice A rationale: Metformin is an antidiabetic medication, and administering it instead of metoprolol may affect the client's glucose levels. Checking the glucose level would help assess the impact and guide further actions.
Choice B rationale: Uric acid levels are not directly affected by metformin or metoprolol.
Choice C rationale: HDL levels are not directly impacted by the accidental administration of metformin instead of metoprolol.
Choice D rationale: Thyroid function levels are not immediately impacted by the accidental administration of metformin instead of metoprolol.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A rationale: Platelet count monitoring is not specific to warfarin therapy; it's essential for other conditions but not primarily for warfarin monitoring.
Choice B rationale: артт (activated partial thromboplastin time) is more relevant for assessing heparin therapy.
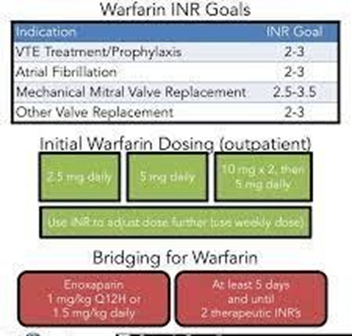
Choice C rationale: INR monitoring is essential for clients on warfarin therapy to assess its anticoagulant effect and maintain therapeutic levels.
Choice D rationale: Fibrinogen monitoring is not specific to warfarin therapy.
Correct Answer is C
Explanation
Choice A rationale: Polyuria (excessive urination) is not a typical manifestation of an allergic reaction to ceftriaxone.
Choice B rationale: Bradycardia is not commonly associated with an allergic reaction to ceftriaxone.
Choice C rationale: Hypotension (low blood pressure) can be a manifestation of an allergic reaction to ceftriaxone. It is crucial for the nurse to recognize this and take appropriate action.
Choice D rationale: Nausea can be a side effect of ceftriaxone but might not solely indicate an allergic reaction.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today