A client who had a biliopancreatic diversion procedure (BPD) 3 months ago is admitted with severe dehydration. Which assessment finding warrants immediate intervention by the nurse?
Gastroccult positive emesis.
Strong foul smelling flatus.
Complaint of poor night vision.
Loose bowel movements.
The Correct Answer is A
Choice A reason: Gastroccult positive emesis indicates the presence of blood in the vomit, which is a sign of a serious complication such as anastomotic leak, ulcer, or bleeding. The nurse should notify the physician and monitor the client's vital signs and hemoglobin level.
Choice B reason: Strong foul smelling flatus is a common side effect of BPD, which involves bypassing a large portion of the small intestine and creating a connection between the stomach and the colon. This results in malabsorption and bacterial overgrowth, which produce gas and odor.
Choice C reason: Complaint of poor night vision is a sign of vitamin A deficiency, which can occur after BPD due to reduced absorption of fat-soluble vitamins. The nurse should advise the client to take vitamin supplements and eat foods rich in vitamin A, such as carrots, sweet potatoes, and spinach.
Choice D reason: Loose bowel movements are another common side effect of BPD, which causes diarrhea and steatorrhea (fatty stools). The nurse should encourage the client to drink fluids with electrolytes and avoid foods that worsen diarrhea, such as greasy, spicy, or sugary foods.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason: This is incorrect because teaching the client to wear a mask, hand wash, and social distance is not the most important action for the nurse to take. These are preventive measures that should be followed by everyone, regardless of their COVID-19 status.
Choice B reason: This is correct because isolating the client from other clients, family, and healthcare workers not wearing proper PPE is the most important action for the nurse to take. This is to prevent transmission of COVID-19 to others who may be at risk of severe complications or death.
Choice C reason: This is incorrect because reporting the COVID-19 result to the local health department according to CDC guidelines is not the most important action for the nurse to take. This is a legal and ethical obligation that should be done after confirming the diagnosis, but it does not have an immediate impact on the client's health or safety.
Choice D reason: This is incorrect because explaining to the client to inform others that they may have been potentially exposed in the last 14 days is not the most important action for the nurse to take. This is a moral and social responsibility that should be done as soon as possible, but it does not address the urgent need of isolating the client from potential sources of infection.
Correct Answer is C
Explanation
Choice A reason: Lifting and clearing drainage from the chest tube is not necessary, as the water level fluctuations indicate that the chest tube is functioning properly and allowing air and fluid to escape from the pleural space.
Choice B reason: Inspecting the tube insertion site for leaking is not indicated, as there is no evidence of air leak in the water-seal chamber. An air leak would cause continuous or intermittent bubbling in the water-seal chamber.
Choice C reason: Continuing to monitor the drainage system is the best action for the nurse to implement, as the water level fluctuations are normal and expected in a water-seal drainage system. The water level should rise during inspiration and fall during expiration, reflecting the changes in intrathoracic pressure.
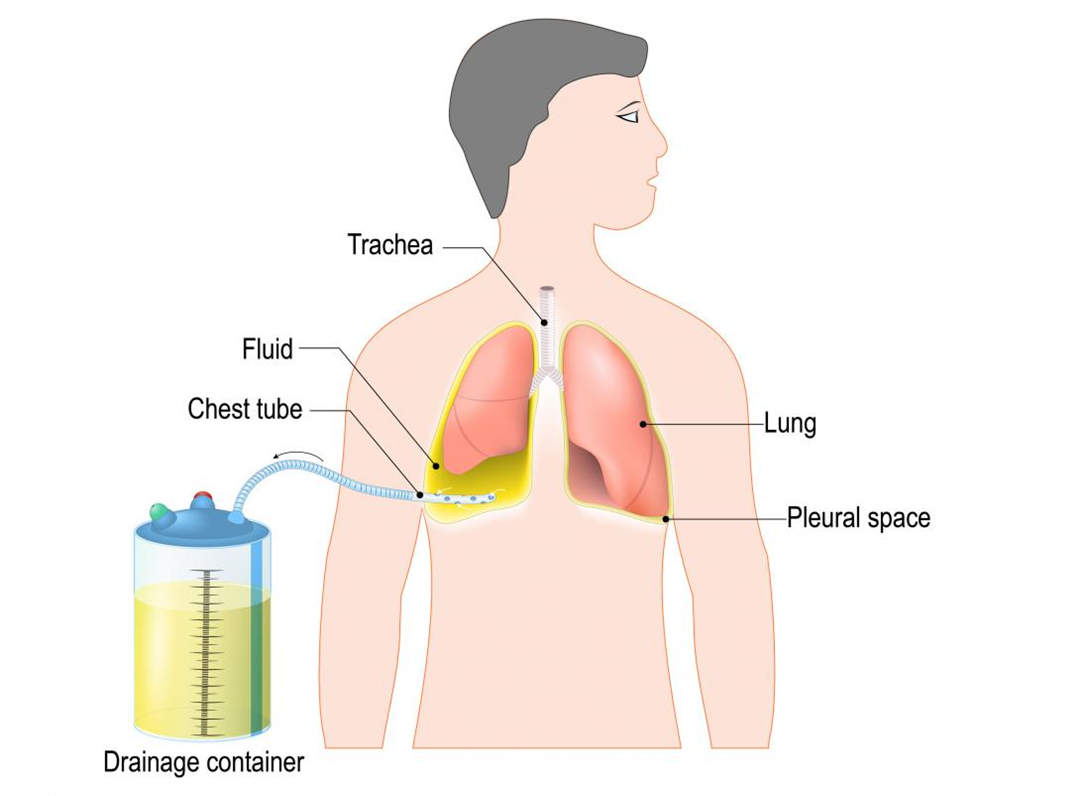
Choice D reason: Auscultating lungs for unequal breath sounds is not relevant, as it does not address the question of what to do with the water level fluctuations. Unequal breath sounds may indicate a pneumothorax or atelectasis, which are complications of chest trauma or chest tube insertion.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today