A client receiving parenteral nutrition by central venous access reports feeling unwell. The nurse assesses the client and suspects that the central line has become infected. Which of the following findings indicate that the client has developed a systemic infection? Select all that apply.
Edema
Purulent drainage at intravenous insertion site
Redness at insertion site
Nausea
Leukocytosis
Fever
Correct Answer : B,E,F
Choice A Reason: Edema is not a specific finding of a systemic infection, but rather a possible sign of fluid overload or impaired venous return. It can occur due to excessive infusion rate, heart failure, or obstruction of blood flow in or around the central line.
Choice B Reason: This is a correct choice. Purulent drainage at intravenous insertion site is a finding of a local infection that can spread systemically. It indicates bacterial invasion and inflammation of the skin and subcutaneous tissue around the catheter.
Choice C Reason: Redness at insertion site is a finding of a local infection that can spread systemically. It indicates increased blood flow and inflammation of the skin and subcutaneous tissue around the catheter.
Choice D Reason: Nausea is not a specific finding of a systemic infection, but rather a possible side effect of parenteral nutrition or a symptom of another condition. It can occur due to electrolyte imbalance, hyperglycemia, or gastrointestinal disorders.
Choice E Reason: This is a correct choice. Leukocytosis is a finding of a systemic infection that indicates increased production and release of white blood cells in response to infection. It can be detected by a blood test.
Choice F Reason: This is a correct choice. Fever is a finding of a systemic infection that indicates increased body temperature due to activation of the immune system and release of pyrogens. It can be measured by a thermometer.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: This is incorrect because it is necessary to remove contact lenses before administering medications. Contact lenses can absorb or interfere with the absorption of eye drops and cause irritation or infection. The nurse should instruct the client to remove contact lenses before applying eye drops and wait at least 15 minutes before reinserting them.
Choice B reason: This is incorrect because administering the medications by touching the tip of the dropper to the sclera of the eye can cause contamination or injury. The sclera is the white part of the eye that covers most of the eyeball. The nurse should instruct the client to avoid touching the tip of the dropper to any part of the eye or eyelid and hold it about 1 cm above the lower eyelid.
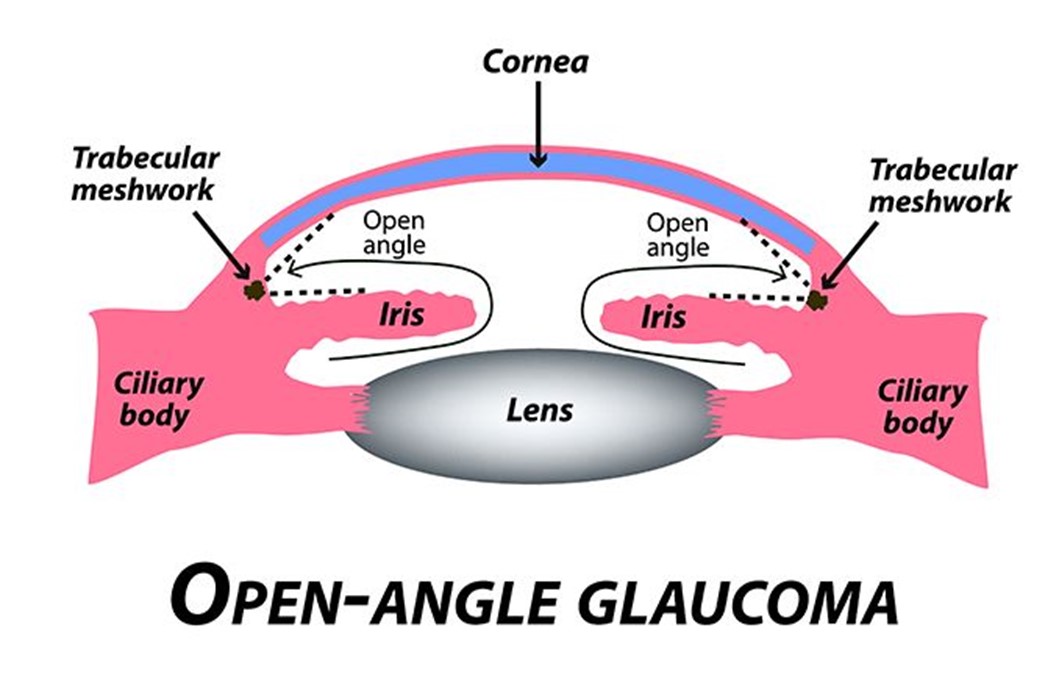
Choice C reason: This is correct because administering the medications 5 min apart can prevent dilution or washout of one medication by another. Timolol and pilocarpine are two different types of eye drops that are used to treat open-angle glaucoma, which is a condition that causes increased pressure inside the eye and damage to the optic nerve. Timolol is a beta-blocker that reduces the production of fluid in the eye, and pilocarpine is a cholinergic agent that increases the drainage of fluid from the eye. The nurse should instruct the client to apply one drop of each medication in the affected eye(s) and wait at least 5 minutes between each medication.
Choice D reason: This is incorrect because holding pressure on the conjunctival sac for 2 min following the application of eye drops can reduce systemic absorption and side effects of eye drops. The conjunctival sac is the space between the lower eyelid and the eyeball. The nurse should instruct the client to gently close their eyes after applying eye drops and press their index finger against the inner corner of their eye for 2 minutes. This can block the tear duct that drains fluid from the eye to the nose and prevent it from entering the bloodstream.
Correct Answer is C
Explanation
Choice A Reason: This choice is incorrect. Inability to read is not a finding that the nurse should expect in a client who has meningitis, but rather a possible finding in a client who has a stroke or a brain tumor. Meningitis does not affect the language or cognitive functions, but rather the meninges or the membranes that cover the brain and spinal cord.
Choice B Reason: This choice is incorrect. Bruising around the eyes is not a finding that the nurse should expect in a client who has meningitis, but rather a possible finding in a client who has a basilar skull fracture or a head trauma. Meningitis does not cause bleeding or bruising, but rather inflammation and infection of the meninges.
Choice C Reason: This is the correct choice. A throbbing headache is a finding that the nurse should expect in a client who has meningitis, as it is one of the most common and characteristic symptoms. A throbbing headache is caused by increased intracranial pressure and irritation of the meninges due to inflammation and infection.
Choice D Reason: This choice is incorrect. A heart rate of 50 is not a finding that the nurse should expect in a client who has meningitis, but rather a possible finding in a client who has bradycardia or a slow heart rate. Meningitis does not affect the heart rate, but rather the temperature and blood pressure. The nurse should expect to see fever and hypotension in a client who has meningitis.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today