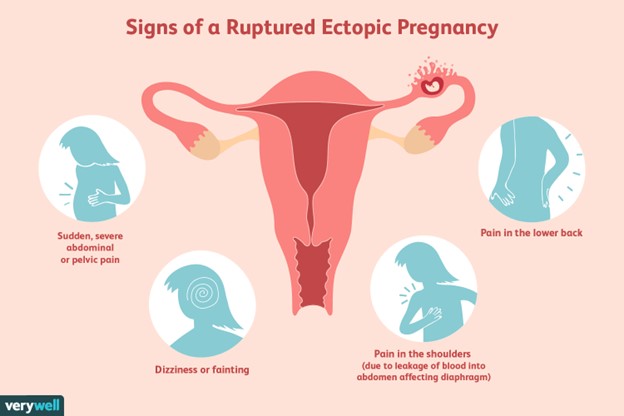
A client is suspected of having a ruptured ectopic pregnancy. Which assessment would the nurse identify as the priority?
Hemorrhage
Edema
Infection
Jaundice
The Correct Answer is A
Choice A reason: Hemorrhage is the most life-threatening complication of a ruptured ectopic pregnancy, as it can lead to hypovolemic shock and death. The nurse should monitor the client's vital signs, blood loss, and level of consciousness, and administer fluids and blood products as ordered.
Choice B reason: Edema is not a common sign of a ruptured ectopic pregnancy, and it is not a priority over hemorrhage. Edema may be caused by other conditions, such as heart failure, kidney disease, or venous insufficiency.
Choice C reason: Infection is a possible complication of a ruptured ectopic pregnancy, but it is not as urgent as hemorrhage. Infection may manifest as fever, chills, malaise, or foul-smelling vaginal discharge. The nurse should administer antibiotics as ordered and monitor the client's temperature and white blood cell count.
Choice D reason: Jaundice is not a typical symptom of a ruptured ectopic pregnancy, and it is not a priority over hemorrhage. Jaundice may indicate liver dysfunction or hemolytic anemia, which are unrelated to ectopic pregnancy. The nurse should assess the client's skin and sclera color, and check the liver enzymes and bilirubin levels.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","D","E","F"]
Explanation
Choice A Reason: Homelessness is a risk factor for high-risk pregnancy because it exposes the woman to various challenges and stressors that can affect her health and well-being. Homeless women may face difficulties in accessing adequate nutrition, hygiene, safety, shelter, transportation, and health care. They may also experience higher levels of violence, substance abuse, mental illness, and social isolation. These factors can increase the risk of infections, complications, preterm birth, low birth weight, and infant mortality.
Choice B Reason: Age is not a risk factor for high-risk pregnancy in this case because the woman is 22 years old, which is within the optimal age range for childbearing. The optimal age range is considered to be between 20 and 35 years old, as women in this age group tend to have fewer complications and better outcomes than women who are younger or older. Women who are younger than 20 or older than 35 are considered to have advanced maternal age or adolescent pregnancy, respectively, which are risk factors for high-risk pregnancy.
Choice C Reason: BP 110/70 is not a risk factor for high-risk pregnancy because it is within the normal range for blood pressure. The normal range for blood pressure is considered to be between 90/60 and 120/80 mmHg. Blood pressure that is too high or too low can indicate problems such as preeclampsia, eclampsia, or hypotension, which are risk factors for high-risk pregnancy.
Choice D Reason: BMI 17.5 is a risk factor for high-risk pregnancy because it indicates that the woman is underweight. BMI stands for body mass index, which is a measure of body fat based on height and weight. The normal range for BMI is considered to be between 18.5 and 24.9 kg/m2. BMI that is too low or too high can indicate problems such as malnutrition, obesity, or gestational diabetes, which are risk factors for high-risk pregnancy.
Choice E Reason: Prenatal care is a risk factor for high-risk pregnancy because it indicates that the woman has not received adequate medical attention and support during her pregnancy. Prenatal care is essential for ensuring the health and well-being of both the mother and the baby. Prenatal care involves regular visits to a health care provider who can monitor the progress of the pregnancy, screen for any complications or infections, provide education and counseling, and prescribe any necessary medications or interventions. Lack of prenatal care can increase the risk of maternal mortality, morbidity, preterm birth, low birth weight, congenital anomalies, and infant mortality.
Choice F Reason: Prenatal history is a risk factor for high-risk pregnancy because it indicates that the woman has had previous pregnancies that ended in miscarriage or stillbirth. Prenatal history can provide important information about the woman's reproductive health and potential complications that may recur or affect her current pregnancy. Previous pregnancy losses can indicate problems such as genetic abnormalities, chromosomal disorders, infections, immunological factors, hormonal imbalances, uterine abnormalities, or placental issues. These factors can increase the risk of spontaneous abortion, fetal demise, preterm birth, intrauterine growth restriction (IUGR), or placenta previa.
Correct Answer is ["A","B","D"]
Explanation
Choice A Reason: This is correct because breast tenderness is a common discomfort during the first trimester of pregnancy. It is caused by hormonal changes that stimulate breast growth and prepare them for lactation. Breast tenderness may also be accompanied by swelling, tingling, or sensitivity.
Choice B Reason: This is correct because urinary frequency is a common discomfort during the first trimester of pregnancy. It is caused by hormonal changes that increase blood flow to the kidneys and bladder, as well as by the growing uterus that puts pressure on the bladder. Urinary frequency may also be associated with increased thirst or urinary tract infections.
Choice C Reason: This is incorrect because backache is not a common discomfort during the first trimester of pregnancy. It usually occurs in later stages of pregnancy, when the weight of the fetus and the uterus shifts the center of gravity and strains the back muscles and ligaments. Backache may also be caused by poor posture, stress, or fatigue.
Choice D Reason: This is correct because cravings are a common discomfort during the first trimester of pregnancy. They are caused by hormonal changes that affect the sense of taste and smell, as well as by emotional or psychological factors. Cravings may vary from person to person and may include foods that are sweet, salty, sour, or spicy.
Choice E Reason: This is incorrect because leg cramps are not a common discomfort during the first trimester of pregnancy. They usually occur in later stages of pregnancy, when there is increased pressure on the nerves and blood vessels that supply the legs. Leg cramps may also be caused by dehydration, electrolyte imbalance, or muscle fatigue.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today