A client who is 4 months pregnant is at the prenatal clinic for her initial visit. Her history reveals she has 7-year-old twins who were born at 34 weeks gestation, a 2-year-old son born at 39 weeks gestation, and a spontaneous abortion 1 year ago at 6 weeks gestation. Using the GTPAL method, the nurse would document her obstetric history as:
3-2-1-0-3
4-1-1-1-3
4-2-1-3-1
3-1-2-2-3
The Correct Answer is B
Choice A Reason: This option is incorrect because it underestimates the number of pregnancies (gravida) and overestimates the number of preterm births (preterm). The client has had four pregnancies (twins count as one pregnancy), not three. The client has had one preterm birth (the twins), not two.
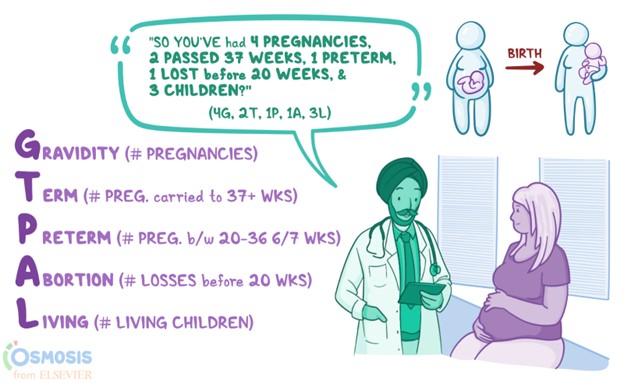
Choice B Reason: This option is correct because it accurately reflects the client's obstetric history. GTPAL stands for Gravida, Term, Preterm, Abortions, and Living children. Gravida is the number of pregnancies a woman has had, regardless of outcome. Term is the number of pregnancies that ended at or beyond 37 weeks gestation. Preterm is the number of pregnancies that ended between 20 and 36 weeks gestation. Abortions are the number of pregnancies that ended before 20 weeks gestation, either spontaneously or induced. Living children are the number of children who are alive at present.
The client has had four pregnancies (gravida), one term birth (the son), one preterm birth (the twins), one abortion (the miscarriage), and three living children (the twins and the son).
Choice C Reason: This option is incorrect because it overestimates the number of preterm births (preterm) and underestimates the number of living children (living). The client has had one preterm birth (the twins), not two. The client has three living children (the twins and the son), not one.
Choice D Reason: This option is incorrect because it underestimates the number of pregnancies (gravida) and overestimates the number of abortions (abortions) and preterm births (preterm). The client has had four pregnancies (twins count as one pregnancy), not three. The client has had one abortion (the miscarriage), not two. The client has had one preterm birth (the twins), not two.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason: This is incorrect because cervical insufficiency is a condition where the cervix dilates prematurely and painlessly during pregnancy, leading to preterm delivery or second trimester abortion. It is not a common cause of first trimester abortion, which occurs before 12 weeks of gestation.
Choice B Reason: This is incorrect because uterine fibroids are benign tumors that grow in or on the uterus. They may cause heavy bleeding, pain, or infertility, but they are not a common cause of first trimester abortion. They may increase the risk of miscarriage in later stages of pregnancy.
Choice C Reason: This is correct because fetal genetic abnormalities are the most common cause of first trimester abortion, accounting for up to 70% of cases. Fetal genetic abnormalities are errors in the number or structure of chromosomes that occur during fertilization or cell division. They can cause developmental defects or fetal demise that result in spontaneous abortion.
Choice D Reason: This is incorrect because maternal disease is not a common cause of first trimester abortion. Maternal disease refers to any medical condition that affects the mother's health or pregnancy outcome, such as diabetes, hypertension, thyroid disorders, or infections. Maternal disease may increase the risk of miscarriage in later stages of pregnancy or cause other complications such as preterm labor or preeclampsia.
Correct Answer is B
Explanation
Choice A Reason: This is incorrect because maternal diabetes is a condition where the mother has high blood sugar levels during pregnancy. It can cause polyhydramnios, or excess amniotic fluid, not oligohydramnios, or low amniotic fluid.
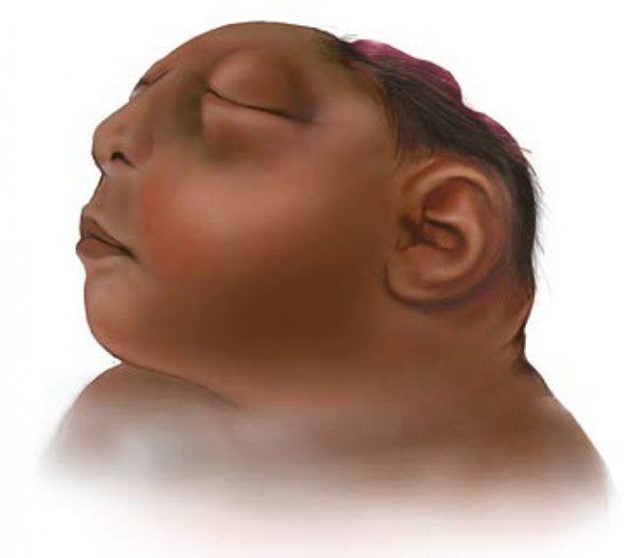
Choice B Reason: This is correct because fetal anencephaly is a congenital defect where the fetus lacks parts of the brain and skull. It can cause oligohydramnios, as the fetus does not produce enough urine to contribute to the amniotic fluid volume.
Choice C Reason: This is incorrect because placental abruption is a complication where the placenta detaches from the uterine wall before delivery. It can cause bleeding, pain, and fetal distress, but not oligohydramnios.
Choice D Reason: This is incorrect because neural tube defects are congenital defects where the spinal cord or brain does not develop properly. They can cause various neurological problems, but not oligohydramnios.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today