A client is admitted with a fever of unknown origin. To assess fever patterns, which intervention should the nurse implement?
Measure temperature at regular intervals.
Assess for flushed, warm skin regularly.
Vary sites for temperature measurement.
Document the client's circadian rhythms.
The Correct Answer is A
Choice A Reason: This is correct because measuring temperature at regular intervals allows the nurse to monitor fever patterns and evaluate the effectiveness of interventions.
Choice B Reason: This is incorrect because assessing for flushed, warm skin regularly is not a reliable indicator of fever. Skin temperature may vary depending on environmental factors and blood flow.
Choice C Reason: This is incorrect because varying sites for temperature measurement may result in inaccurate readings. Different sites have different normal ranges and may be affected by external factors.
Choice D Reason: This is incorrect because documenting the client's circadian rhythms is not relevant to assessing fever patterns. Circadian rhythms are natural fluctuations in body functions that occur over a 24-hour cycle.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
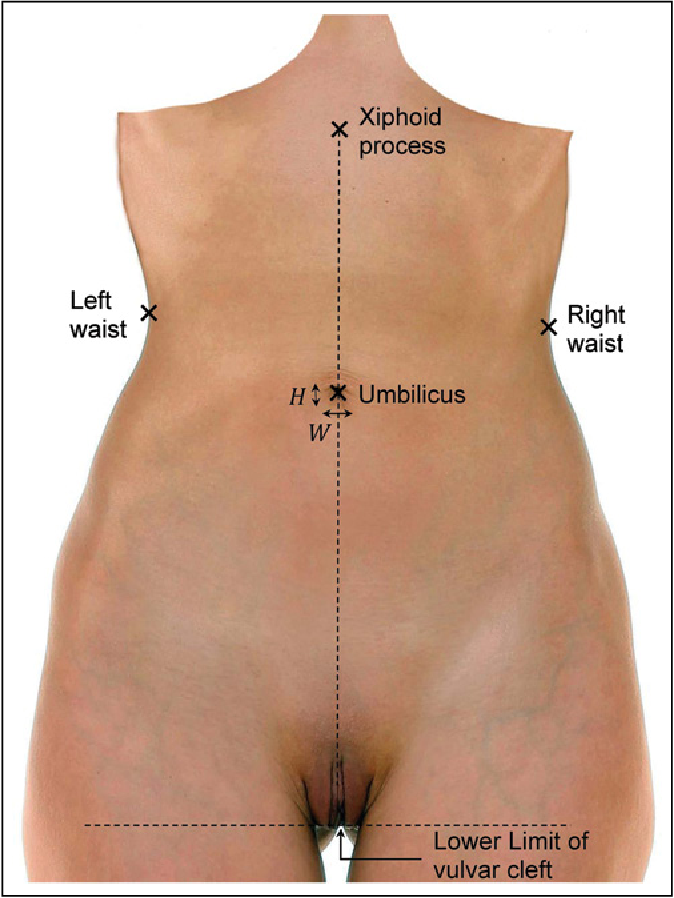
Choice A: Massage the injection site to increase absorption is not a correct instruction because it may cause bruising and bleeding. Low-molecular-weight heparin is absorbed quickly without massaging.
Choice B: Rotate injections between the abdomen and gluteal areas is not a correct instruction because it may increase the risk of hematoma and infection. The abdomen is preferred over other sites for low-molecular-weight heparin injections.
Choice C: Expel the air in the prefilled syringe prior to injection is not a correct instruction because it may result in loss of medication and inaccurate dosing. The air bubble in the prefilled syringe should be left intact.
Choice D: Inject in abdominal area at least 2 inches from the umbilicus is a correct instruction because it ensures adequate subcutaneous tissue and avoids major blood vessels and organs.
Correct Answer is C
Explanation
Choice A Reason: This is incorrect because regular exercise is a beneficial lifestyle modification for preventing and managing cardiac disease, but it is not the most important one. Smoking cessation has a greater impact on reducing the risk of cardiovascular events and mortality.
Choice B Reason: This is incorrect because stress reduction is a helpful lifestyle modification for preventing and managing cardiac disease, but it is not the most important one. Smoking cessation has a more direct effect on improving the function and structure of the blood vessels and heart.
Choice C Reason: This is correct because smoking cessation is the most important lifestyle modification for preventing and managing cardiac disease, as smoking is a major modifiable risk factor that can cause atherosclerosis, hypertension, arrhythmias, thrombosis, and myocardial infarction.
Choice D Reason: This is incorrect because a low-fat diet is a useful lifestyle modification for preventing and managing cardiac disease, but it is not the most important one. Smoking cessation has a stronger influence on lowering the levels of cholesterol and inflammation in the blood.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today