After an intravenous antibiotic is started, the nurse determines that the medication is not prescribed for the client and stops the infusion. Which action should the nurse implement next?
Notify the healthcare provider.
Document the event on the chart.
Complete an incident report.
Inform the nurse on the next shift.
The Correct Answer is A
Choice A: Notify the healthcare provider is the correct action because it is the nurse's responsibility to report any medication errors or adverse reactions to the prescriber as soon as possible.
Choice B: Document the event on the chart is not the next action because it should be done after notifying the healthcare provider and completing an incident report.
Choice C: Complete an incident report is not the next action because it should be done after notifying the healthcare provider and before documenting the event on the chart.
Choice D: Inform the nurse on the next shift is not the next action because it should be done after documenting the event on the chart and during handoff.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A: Massage the injection site to increase absorption is not a correct instruction because it may cause bruising and bleeding. Low-molecular-weight heparin is absorbed quickly without massaging.
Choice B: Rotate injections between the abdomen and gluteal areas is not a correct instruction because it may increase the risk of hematoma and infection. The abdomen is preferred over other sites for low-molecular-weight heparin injections.
Choice C: Expel the air in the prefilled syringe prior to injection is not a correct instruction because it may result in loss of medication and inaccurate dosing. The air bubble in the prefilled syringe should be left intact.
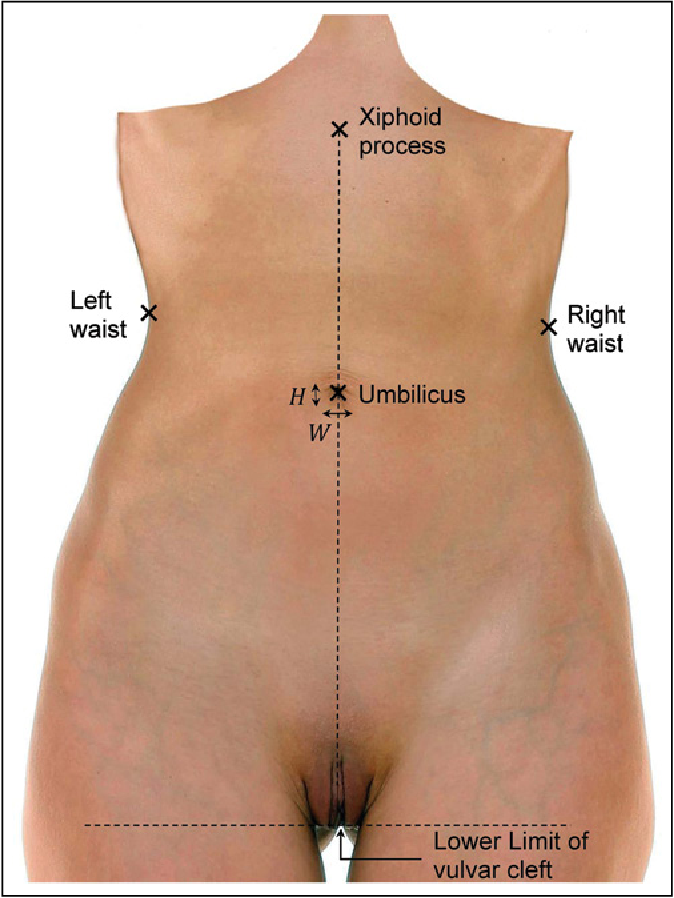
Choice D: Inject in abdominal area at least 2 inches from the umbilicus is a correct instruction because it ensures adequate subcutaneous tissue and avoids major blood vessels and organs.
Correct Answer is B
Explanation
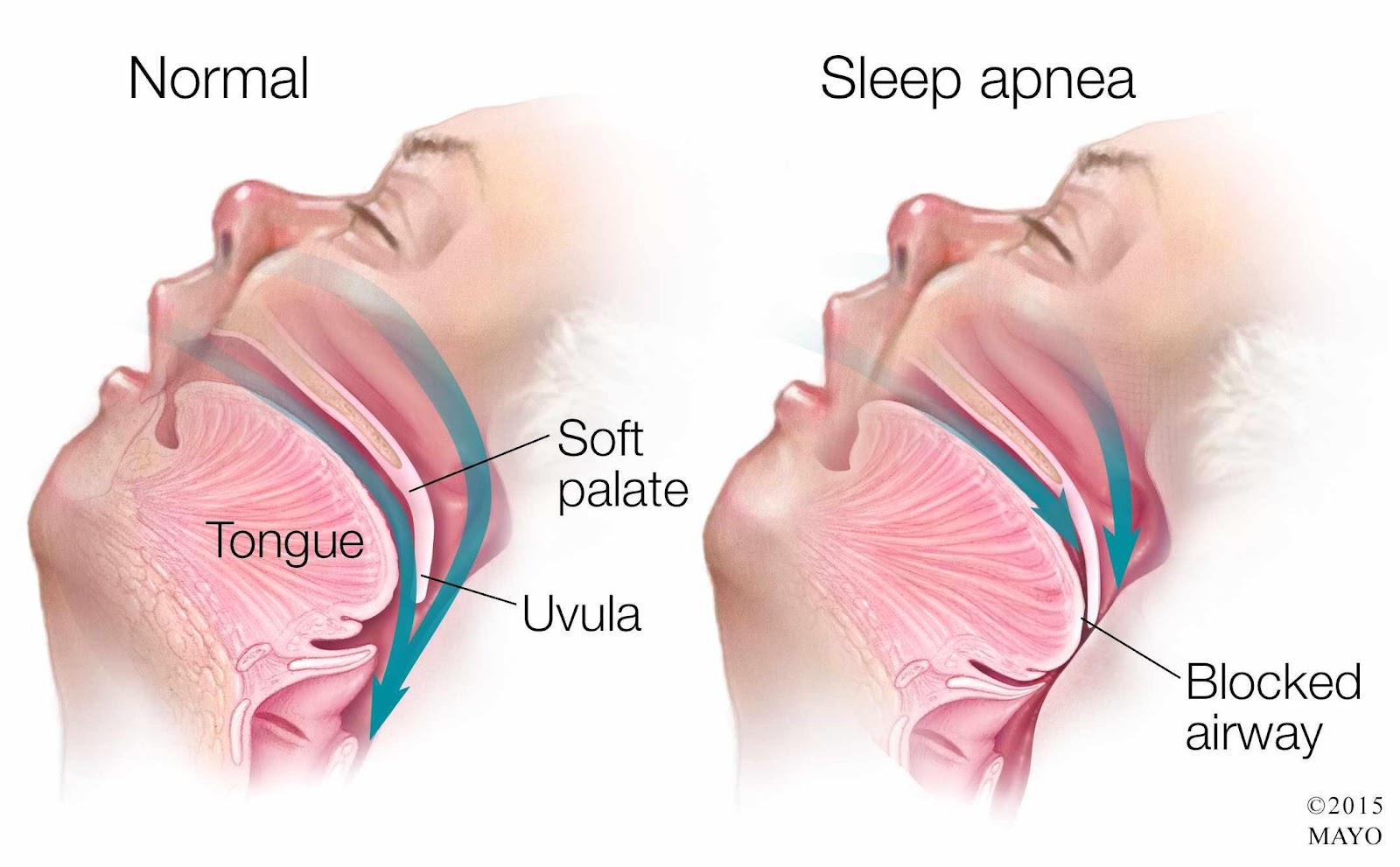
Choice A Reason: This is incorrect because lifting and locking the side rails in place is a standard safety measure for all clients, but it does not address the specific risk of respiratory depression caused by morphine and OSA.
Choice B Reason: This is correct because applying the client's positive airway pressure device can help maintain airway patency and prevent hypoxia and hypercapnia, which are common complications of OSA and opioid use.
Choice C Reason: This is incorrect because elevating the head of the bed to a 45-degree angle can help reduce chest pain and dyspnea, but it does not prevent airway obstruction or respiratory depression.
Choice D Reason: This is incorrect because removing dentures or other oral appliances can help prevent aspiration, but it does not affect the client's breathing pattern or oxygenation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today