A client arrives to the emergency department after losing consciousness during a soccer game. Which of the following actions should the nurse take first?
Prepare the client for an X-Ray.
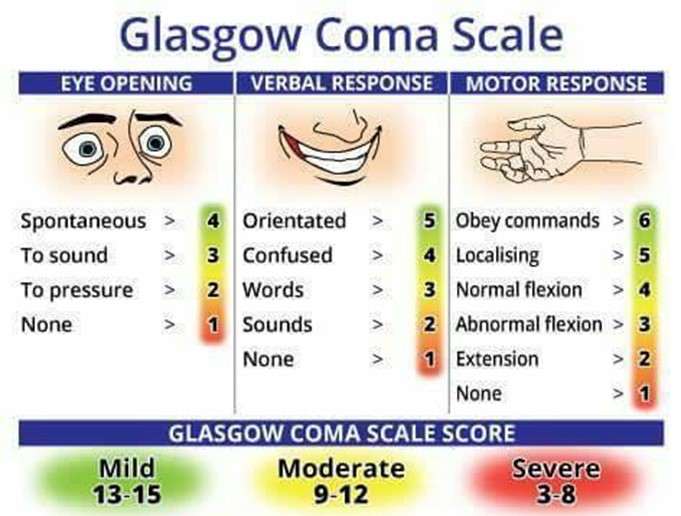
Calculate a Glasgow Coma Score.
Dim the lights and turn off the TV.
Provide analgesics.
The Correct Answer is B
Choice A reason: This is incorrect because preparing the client for an X-ray is not the first action that the nurse should take. An X-ray can help diagnose possible injuries or fractures, but it is not an urgent test. The nurse should first assess the client's level of consciousness and neurological status using a standardized tool such as the Glasgow Coma Scale.
Choice B reason: This is the correct answer because calculating a Glasgow Coma Score is the first action that the nurse should take. The Glasgow Coma Scale is a tool that measures the level of consciousness based on the eye-opening, verbal response, and motor responses. It can help determine the severity of brain injury and guide further interventions.
Choice C reason: This is incorrect because dimming the lights and turning off the TV are not the first actions that the nurse should take. These are environmental modifications that can help reduce sensory stimulation and prevent agitation or seizures, but they are not as important as assessing the level of consciousness and neurological status.
Choice D reason: This is incorrect because providing analgesics is not the first action that the nurse should take. Analgesics can help relieve pain and discomfort, but they can also alter the level of consciousness and mask neurological signs. The nurse should first assess the level of consciousness and neurological status, and then administer analgesics as prescribed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason: This is incorrect because inability to recognize any words may indicate a problem with the auditory cortex, which is the part of the brain that processes sound, not the inner ear. The inner ear consists of the cochlea, which converts sound waves into nerve impulses, and the vestibular system, which helps with balance and orientation.
Choice B Reason: This is correct because loss of balance is a common symptom of an inner ear infection. An inner ear infection can cause inflammation and fluid buildup in the vestibular system, which can disrupt the sense of equilibrium and cause vertigo, dizziness, or nausea.
Choice C Reason: This is incorrect because twitching of the cheek may indicate a problem with the facial nerve, which controls the muscles of facial expression, not the inner ear. The facial nerve runs close to the inner ear, but it is not part of it.
Choice D Reason: This is incorrect because lack of air sound may indicate a problem with the outer or middle ear, which transmit sound waves to the inner ear, not the inner ear itself. The outer ear consists of the pinna and the ear canal, and the middle ear consists of the eardrum and the ossicles.
Correct Answer is A
Explanation
Choice A reason: This is correct because the lesion on the child's head is most likely a hemangioma, which is a benign tumor of blood vessels that appears as a red or purple mark on the skin. Hemangiomas are common in newborns and usually grow during the first year of life, then shrink and fade over several years. The nurse should reassure the client that hemangiomas are harmless and do not require treatment unless they interfere with vision, breathing, or feeding.
Choice B reason: This is incorrect because the lesion on the child's head will not spread, but rather grow and shrink within a limited area. The nurse should not alarm the client by suggesting that the lesion will spread to other parts of the body or become malignant. The nurse should explain that hemangiomas are not contagious or infectious and do not affect the child's overall health or development.
Choice C reason: This is incorrect because the lesion on the child's head is not caused by scarring from the birth process, but rather by abnormal growth of blood vessels in the skin. The nurse should not confuse or misinform the client about the cause of the lesion. The nurse should explain that hemangiomas are not related to trauma, infection, or genetics, but rather to unknown factors that influence blood vessel formation during fetal development.
Choice D reason: This is incorrect because the lesion on the child's head is not a precancerous lesion and does not need a referral to a dermatologist. The nurse should not scare or mislead the client by suggesting that the lesion is a sign of cancer or requires further evaluation or treatment. The nurse should explain that hemangiomas are benign and usually resolve on their own without any complications or sequelae.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today