A charge nurse in a long-term care facility notices the smell of alcohol on a nurse's breath. Which of the following actions should the nurse take first?
Document objective findings about the situation.
Assign clients to the remaining staff.
Call the supervisor to ask for another nurse.
Remove the nurse from the client care area.
The Correct Answer is D
Choice A Reason:
Document objective findings about the situation is incorrect. While documentation is important, it should not be the first action when the charge nurse suspects a colleague is under the influence of alcohol. Patient safety takes precedence, and immediate action to remove the nurse from patient care is necessary to prevent potential harm.
Choice B Reason;
Assigning clients to the remaining staff is incorrect. Assigning clients to other staff members is an appropriate step but should come after the nurse under suspicion has been removed from patient care to ensure their safety. Patient safety is the primary concern.
Choice C Reason:
Calling the supervisor to ask for another nurse is incorrect. Contacting the supervisor is a reasonable action, but it should be done after the immediate safety concern has been addressed by removing the nurse from patient care. This allows the supervisor to be informed of the situation and take appropriate action.
Choice D Reason:
Removing the nurse from the client care area is correct.When a charge nurse detects the smell of alcohol on a nurse's breath, the first and most immediate action should be to remove the nurse from the client care area to ensure patient safety. Alcohol impairment can severely compromise a nurse's ability to provide safe and effective care. Once the nurse is removed from patient care, further actions, such as documenting objective findings and contacting the supervisor, can be taken to address the situation and ensure appropriate follow-up, including any necessary interventions or investigations. Patient safety should always be the top priority in such situations.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason:
An occupational therapist focuses on helping clients develop or regain skills needed for daily living and working, but transportation coordination is typically not within their primary scope.
Choice B Reason:
Physical therapist is incorrect. While physical therapists play a crucial role in rehabilitation and mobility, their primary focus is on improving physical function, strength, and mobility. They do not typically assess or address driving-related concerns.
Choice C Reason:
A social worker can assist the client in arranging transportation to follow-up appointments. They can connect the client with community resources, transportation services, or support systems that can help with these needs.
Choice D Reason:
Primary care provider is incorrect. While a primary care provider can discuss general health concerns, they may not have the expertise or resources to assess and address specific driving-related issues or provide driving rehabilitation.
Correct Answer is D
Explanation
Choice A Reason:
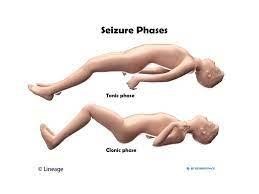
Restraining the child's upper extremities is not recommended. It's important to allow the child to move freely during the seizure to prevent injury. Attempting to restrain their movements could result in harm to the child or the person attempting to restrain them.
Choice B Reason:
Turning the child onto their back is generally appropriate as long as you do it gently and without force. It helps ensure that the airway remains clear and allows any fluids to drain out of the mouth. However, you should not forcibly turn the child; instead, gently guide them if necessary.
Choice C Reason:
Placing a padded tongue blade or any object in the child's mouth is strongly discouraged during a seizure. Doing so can result in injury to the child's mouth, teeth, or jaw. It is a common misconception that someone might swallow their tongue during a seizure, but this rarely happens. It's essential to keep the child's airway clear but not to insert any objects into their mouth.
D. Placing a pillow under the child's head is appropriate to protect their head from injury, especially if they are on a hard surface. It can help cushion the head and reduce the risk of head trauma during the seizure.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today