Which position should a nurse instruct a patient to assume after a lumbar puncture to prevent a headache?
Lie flat.
Lie on left side.
Stay in semi-Fowler position.
Ambulate in the room with assistance.
The Correct Answer is A
A. Lie flat:
This option involves instructing the patient to lie flat on their back without elevating their head. Lying flat helps to maintain consistent pressure in the spinal canal, reducing the likelihood of CSF leakage from the puncture site. This position is commonly recommended after a lumbar puncture to prevent or minimize the occurrence of post-lumbar puncture headaches (PLPH).
B. Lie on left side:
This option involves instructing the patient to lie on their left side. While lying on the left side may provide some relief by reducing pressure on the lumbar puncture site, it is not typically recommended immediately after the procedure to prevent PLPH. Lying flat is generally preferred to minimize changes in CSF pressure and reduce the risk of headache.
C. Stay in semi-Fowler position:
The semi-Fowler position involves elevating the head of the bed at a 30-45 degree angle. This position is not typically recommended immediately after a lumbar puncture because it may increase CSF leakage and pressure changes, potentially exacerbating the risk of developing a headache.
D. Ambulate in the room with assistance:
Ambulating shortly after a lumbar puncture is not typically recommended as it may increase the risk of developing a headache. Movement and changes in posture can exacerbate CSF leakage and pressure changes at the puncture site, leading to the development of post-lumbar puncture headaches.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","B","C","D","E","F"]
Explanation
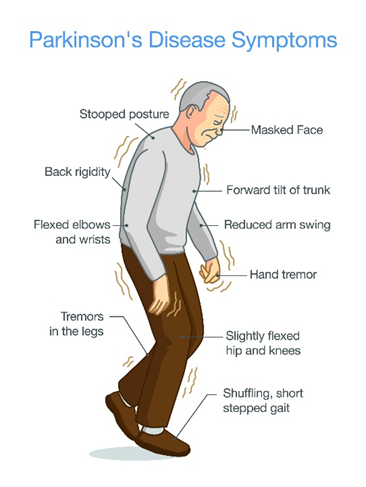
A. Muscle tremors:
Muscle tremors, particularly resting tremors, are a hallmark feature of Parkinson's disease. These tremors typically occur in the hands, fingers, arms, legs, jaw, or head and may worsen with stress or inactivity.
B. Slow body movement (bradykinesia):
Bradykinesia refers to slowness of movement and is another key symptom of Parkinson's disease. Patients may have difficulty initiating movement, experience a decrease in spontaneous movement (hypokinesia), and demonstrate reduced range of motion.
C. Rigidity:
Rigidity, or stiffness of the muscles, is a common symptom of Parkinson's disease. It often affects the limbs and trunk and can contribute to difficulty with movement and posture.
D. Pill rolling:
Pill rolling refers to a specific type of tremor characterized by rhythmic, rolling movements of the thumb and fingers, resembling the action of rolling a pill between the fingers and thumb. This tremor is commonly seen in Parkinson's disease.
E. Lack of facial expression:
Parkinson's disease can lead to a reduced range of facial expressions, also known as hypomimia or "masked facies." Patients may have a fixed, expressionless facial appearance and reduced blinking.
F. Drooling:
Drooling, or excessive salivation, can occur in Parkinson's disease due to impaired swallowing function (dysphagia) and reduced control over oral and facial muscles.
Correct Answer is C
Explanation
A.While monitoring for elevated blood pressure is important in identifying autonomic dysreflexia once it occurs, it does not prevent the condition. The nurse should focus on eliminating potential triggers, such as bladder distention or constipation, to prevent the occurrence.
B.Headaches are a symptom of autonomic dysreflexia, often related to severe hypertension. While treating the headache may alleviate discomfort, it does not address the underlying cause, nor does it prevent the onset of autonomic dysreflexia.
C.Bladder distention is a common trigger for autonomic dysreflexia in individuals with spinal cord injuries. The nurse should ensure that the client's bladder is regularly emptied to prevent overdistention, which can stimulate the autonomic reflex and trigger AD.
D.Elevating the head is an intervention used during an episode of autonomic dysreflexia to help lower blood pressure and reduce symptoms. However, this action does not prevent the condition from occurring.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today