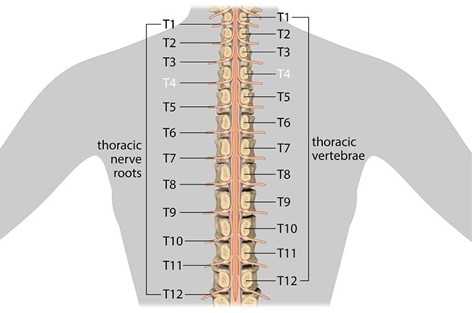
A nurse is caring for a client who has a spinal cord injury at T-4. The nurse should recognize that the client is at risk for autonomic dysreflexia. Which of the following interventions should the nurse take to prevent autonomic dysreflexia?
Monitor for elevated blood pressure.
Provide analgesia for headaches.
Prevent bladder distention.
Elevate the client's head.
The Correct Answer is C
To prevent autonomic dysreflexia, the nurse should take the intervention of preventing bladder distention. Autonomic dysreflexia is a serious medical problem that can happen if a person has injured the spinal cord in their upper back¹. It makes their blood pressure dangerously high and can lead to a stroke, seizure, or cardiac arrest¹. One way to lower the chance of complications is to use the bathroom on a regular schedule and keep the bladder and bowels from becoming too full.
a. Monitoring for elevated blood pressure is important but not an intervention to prevent autonomic dysreflexia.
b. Providing analgesia for headaches is important but not an intervention to prevent autonomic dysreflexia.
d. Elevating the client's head is important but not an intervention to prevent autonomic dysreflexia.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
The nurse should immediately report small drops of clear fluid in the left ear to the charge nurse. This finding could indicate a cerebrospinal fluid (CSF) leak, which can occur as a result of a head injury. A CSF leak can be a serious medical condition that requires immediate attention.
An edematous bruise on the forehead, client disorientation to place, and a heart rate of 110/min and regular are also important findings that the nurse should report to the charge nurse. However, these findings are not as urgent as the presence of small drops of clear fluid in the left ear.

Correct Answer is C
Explanation
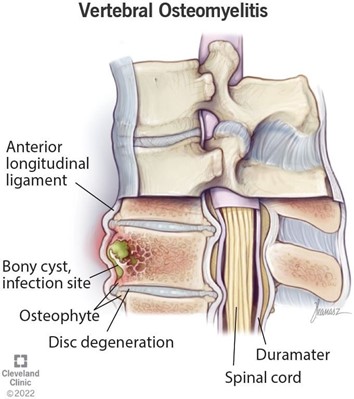
The priority intervention for the nurse to implement for a newly-admitted client who has acute osteomyelitis is antibiotic therapy. Osteomyelitis is an inflammatory condition of bone secondary to an infectious process¹. Antibiotics are the primary treatment option and should be tailored based on culture results and individual patient factors.
a. Optimal nutrition and hydration is important but not the priority intervention.
b. Surgical debridement of necrotic tissue may be necessary but is not the priority intervention.
d. Antipyretic therapy may be necessary but is not the priority intervention.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today