Which client is at the greatest risk for pressure injury development?
A 44yearold prescribed antibiotics for pneumonia
A 26yearold bedridden client with a fractured leg
A 65yearold with hemiparesis and incontinence
A 78yearold requiring assistance to ambulate with a walker
The Correct Answer is C
Choice A reason: A 44yearold prescribed antibiotics for pneumonia is not at the greatest risk for pressure injury development, because he or she does not have any major risk factors for pressure injury. Pressure injury is a localized damage to the skin and underlying tissues caused by pressure, shear, friction, or moisture. Antibiotics for pneumonia do not directly affect the skin integrity or blood circulation, nor do they impair the mobility or sensation of the client.
Choice B reason: A 26yearold bedridden client with a fractured leg is at a high risk for pressure injury development, but not the greatest, because he or she has only one major risk factor for pressure injury. Bedridden status is a major risk factor for pressure injury, because it causes prolonged pressure on the bony prominences, such as the sacrum, heels, or hips, which can impair blood flow and oxygen delivery to the skin and tissues. However, the client's age, fracture, and mobility may mitigate some of the risk, as he or she may have better skin elasticity, wound healing, and ability to reposition.
Choice C reason: A 65yearold with hemiparesis and incontinence is at the greatest risk for pressure injury development, because he or she has multiple major risk factors for pressure injury. Age is a risk factor for pressure injury, because it causes decreased skin elasticity, thickness, and vascularity, which can affect the skin's resilience and repair. Hemiparesis is a risk factor for pressure injury, because it causes reduced mobility, sensation, and muscle mass, which can affect the client's ability to reposition, feel pain, and maintain tissue perfusion. Incontinence is a risk factor for pressure injury, because it causes moisture, irritation, and infection of the skin, which can weaken the skin barrier and delay wound healing.
Choice D reason: A 78yearold requiring assistance to ambulate with a walker is at a moderate risk for pressure injury development, but not the greatest, because he or she has only one major risk factor for pressure injury. Age is a risk factor for pressure injury, as explained above. However, the client's ambulation and assistance may reduce some of the risk, as he or she may have less pressure, shear, and friction on the skin and tissues, and more blood circulation and oxygen delivery.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: Calling the chaplain for support is not the priority nursing intervention for a client who speaks only Spanish. The chaplain may not be able to communicate with the client or understand their needs. This choice does not address the language barrier or the client's reason for admission.
Choice B reason: Verifying the reason for admission is an important nursing intervention, but it is not the priority for a client who speaks only Spanish. The nurse cannot verify the reason for admission without communicating with the client or their family. This choice does not address the language barrier or the client's safety.
Choice C reason: Requesting a medical interpreter is the priority nursing intervention for a client who speaks only Spanish. The medical interpreter can facilitate communication between the nurse and the client, and help the nurse assess the client's condition, reason for admission, and needs. This choice addresses the language barrier and the client's safety.
Choice D reason: Giving the client a tour of the unit is not the priority nursing intervention for a client who speaks only Spanish. The client may not understand the tour or the information given by the nurse. This choice does not address the language barrier or the client's reason for admission.
Correct Answer is C
Explanation
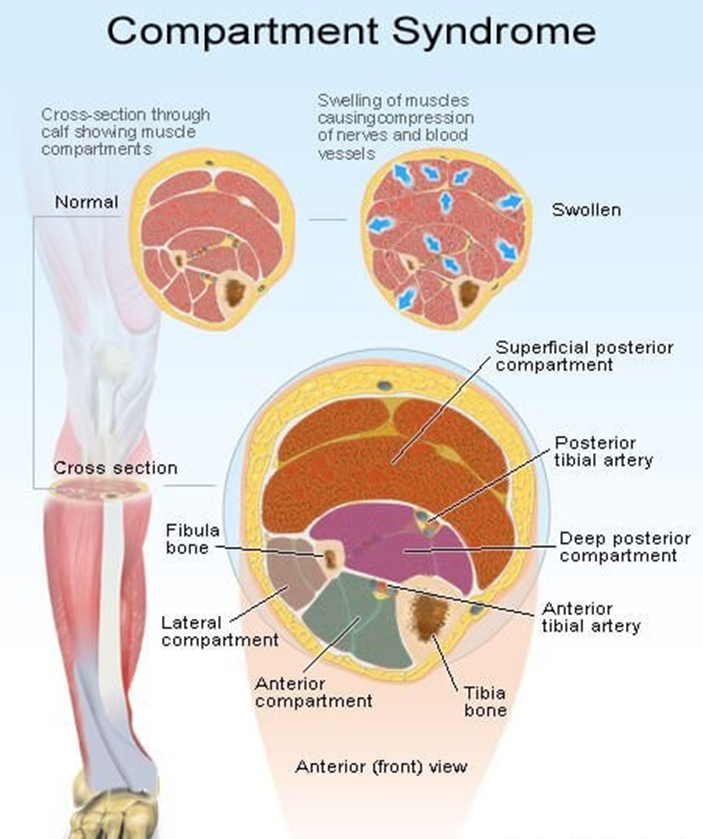
Choice A reason: A bone fragment has injured the nerve supply in the area is not the best response by the nurse. This may be a possible complication of a fracture, but it does not explain the mechanism of compartment syndrome. Compartment syndrome is a condition where the pressure within a closed space (such as a muscle compartment) exceeds the perfusion pressure and causes ischemia and necrosis of the tissues. A bone fragment may damage the nerve, but it does not cause increased pressure in the compartment.
Choice B reason: An injured artery causes impaired arterial perfusion through the compartment is not the best response by the nurse. This may be a possible cause of compartment syndrome, but it is not the most common one. Compartment syndrome is more often caused by venous obstruction than arterial obstruction. An injured artery may reduce the blood flow to the compartment, but it does not cause increased pressure in the compartment.
Choice C reason: Bleeding and swelling cause increased pressure in an area that cannot expand is the best response by the nurse. This is the most common cause of compartment syndrome and explains the pathophysiology of the condition. Bleeding and swelling are the result of inflammation and tissue injury that occur after a fracture. They increase the volume of fluid in the compartment, which cannot expand due to the rigid fascia that surrounds it. This leads to increased pressure in the compartment, which compresses the blood vessels, nerves, and muscles and causes ischemia and necrosis of the tissues.
Choice D reason: The fascia expands with injury, causing pressure on underlying nerves and muscles is not the best response by the nurse. This is not a correct statement, as the fascia does not expand with injury. The fascia is a tough connective tissue that encloses the muscle compartments and limits their expansion. The fascia is part of the problem, not the cause, of compartment syndrome. The fascia prevents the compartment from accommodating the increased volume of fluid and causes increased pressure in the compartment.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today