What is the priority nursing goal for a 14-year-old diagnosed with Graves’ disease?
Relieving constipation
Allowing the adolescent to make decisions about whether or not to take medication
Verbalizing the importance of monitoring for medication side effects
Developing alternative educational goals
The Correct Answer is C
Verbalizing the importance of monitoring for medication side effects.
Graves’ disease is an autoimmune disorder that causes hyperthyroidism, which means the thyroid gland produces too much thyroid hormone. This can lead to symptoms such as weight loss, increased appetite, nervousness, irritability, insomnia, heat intolerance, and palpitations. The medication methimazole is used to treat Graves’ disease by blocking the synthesis of thyroid hormone. However, methimazole can also cause serious side effects such as liver damage, agranulocytosis (low white blood cell count), and allergic reactions.
Therefore, the priority nursing goal for a 14 year old diagnosed with Graves’ disease is to verbalize the importance of monitoring for medication side effects and reporting them to the health care provider.
Choice A is wrong because relieving constipation is not a priority goal for Graves’ disease. Constipation is more likely to occur in hypothyroidism, which is the opposite of hyperthyroidism.
Choice B is wrong because allowing the adolescent to make decisions about whether or not to take medication is not a priority goal for Graves’ disease. While it is important to respect the adolescent’s autonomy and involve them in their care plan, they also need to understand the risks and benefits of taking medication and the consequences of not taking it.
Choice D is wrong because developing alternative educational goals is not a priority goal for Graves’ disease. Graves’ disease can affect the academic performance of adolescents due to cognitive and emotional changes caused by hyperthyroidism.
However, this does not mean that they need to change their educational goals. They may need extra support and accommodations from their teachers and parents to cope with their condition and achieve their potential.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Chronic otitis media with effusion (OME) is a condition where fluid accumulates in the middle ear without signs of infection.
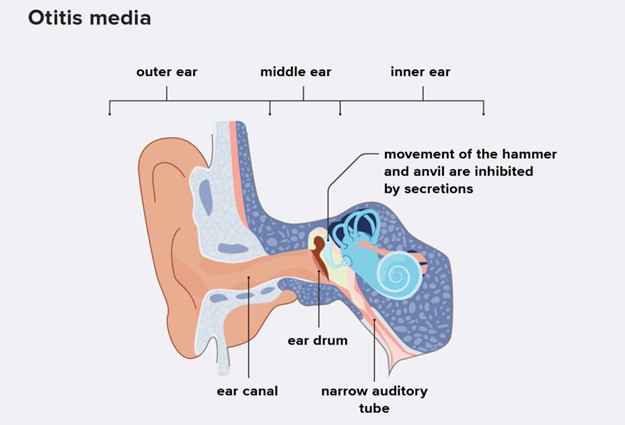
This can cause hearing loss, speech delay, and balance problems. The child may complain of a feeling of fullness or pressure in the ear.
Choice A is wrong because a fever as high as 40° C (104° F) is a sign of acute otitis media, which is an infection of the middle ear with inflammation and pus formation.
Choice B is wrong because severe pain in the ear is also a sign of acute otitis media, not chronic otitis media with effusion.
Choice C is wrong because nausea and vomiting are not typical symptoms of chronic otitis media with effusion. They may be associated with other conditions such as gastroenteritis or vestibular disorders.
Correct Answer is D
Explanation
Therapeutic management includes the administration of gamma globulin and aspirin. This is because Kawasaki disease causes inflammation in the walls of small to medium-sized blood vessels that carry blood throughout the body and can lead to complications such as coronary artery aneurysms. Gamma globulin is an intravenous immunoglobulin that can reduce the risk of these complications, and aspirin can help lower fever and inflammation.
Choice A is wrong because the child’s fever is usually not responsive to antibiotics within 48 hours. Kawasaki disease is not caused by a bacterial infection, so antibiotics are not effective.
Choice B is wrong because the principal area of involvement is not the joints. Kawasaki disease affects mainly the blood vessels, but it can also cause swelling in glands (lymph nodes) and mucous membranes inside the mouth, nose, eyes and throat. Joint pain or swelling may occur, but it is not the main feature of the disease.
Choice C is wrong because aspirin is not contraindicated. Aspirin is part of the standard treatment for Kawasaki disease, along with gamma globulin. However, aspirin should be used with caution and under medical supervision, as it can cause Reye’s syndrome in children with viral infections.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today