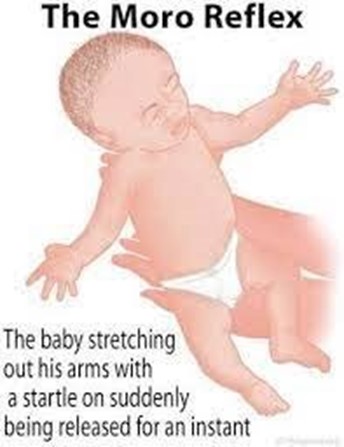
The nurse is performing a newborn physical assessment and is about to elicit the Moro reflex. Which of the following responses should the nurse expect to see?
Select one:
The cheek of the newborn is touched, and the newborn turns toward the side that was touched.
The newborn is suddenly lowered or startled, and they extend their arms, legs and neck, then rapidly bring their arms together.
The newborn is supine and their head is turned to one side, then the arm on that same side extends.
The lateral aspect of the sole of the newborn's foot is stroked, and the toes extend and fan outward.
The Correct Answer is B
Choice A Reason: The cheek of the newborn is touched, and the newborn turns toward the side that was touched. This is an incorrect answer that describes a different reflex called the rooting reflex. The rooting reflex is a feeding reflex that helps the newborn locate the nipple and initiate sucking. The rooting reflex is elicited by stroking the cheek or corner of the mouth of the newborn, which causes them to turn their head and open their mouth toward the stimulus.
Choice B Reason: The newborn is suddenly lowered or startled, and they extend their arms, legs and neck, then rapidly bring their arms together. This is because this response describes the Moro reflex, which is a primitive reflex that is present at birth and disappears by 3 to 6 months of age. The Moro reflex is elicited by simulating a falling sensation or a loud noise, which triggers a fear response in the newborn. The Moro reflex consists of four phases: extension, abduction, adduction, and crying.
Choice C Reason: The newborn is supine and their head is turned to one side, then the arm on that same side extends. This is an incorrect answer that refers to another reflex called the tonic neck reflex. The tonic neck reflex is a postural reflex that helps prepare the newborn for voluntary reaching. The tonic neck reflex is elicited by placing the newborn in a supine position and turning their head to one side, which causes them to assume a "fencing" posture with one arm extended and one arm flexed.
Choice D Reason: The lateral aspect of the sole of the newborn's foot is stroked, and the toes extend and fan outward. This is an incorrect answer that indicates a different reflex called the Babinski reflex. The Babinski reflex is a neurological reflex that tests for spinal cord integrity. The Babinski reflex is elicited by stroking the lateral aspect of the sole of the foot from heel to toe, which causes the big toe to dorsiflex and the other toes to fan out.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A Reason: Respiratory rate of 16. This is an incorrect answer that indicates a normal finding that does not suggest magnesium sulfate toxicity. Respiratory rate is a measure of the number of breaths per minute, which reflects the respiratory function and oxygenation status. Respiratory rate of 16 is within the normal range for adults, which is 12 to 20 breaths per minute. Respiratory rate of 16 does not indicate magnesium sulfate toxicity, which can cause respiratory rate below 12 breaths per minute.
Choice B Reason: Complaints by the client of feeling flushed and warm. This is an incorrect answer that indicates a common side effect that does not indicate magnesium sulfate toxicity. Feeling flushed and warm are sensations that are caused by vasodilation (widening of blood vessels), which can occur as a result of magnesium sulfate administration. Feeling flushed and warm are not signs of magnesium sulfate toxicity, but rather expected and mild reactions that usually subside within a few hours.
Choice C Reason: Fetal heart rate of 120. This is an incorrect answer that indicates a normal finding that does not suggest magnesium sulfate toxicity. Fetal heart rate is a measure of the number of beats per minute of the fetal heart, which reflects the fetal well-being and oxygenation status. Fetal heart rate of 120 is within the normal range for fetuses, which is 110 to 160 beats per minute. Fetal heart rate of 120 does not indicate magnesium sulfate toxicity, which can cause fetal heart rate below 110 beats per minute or above 160 beats per minute.
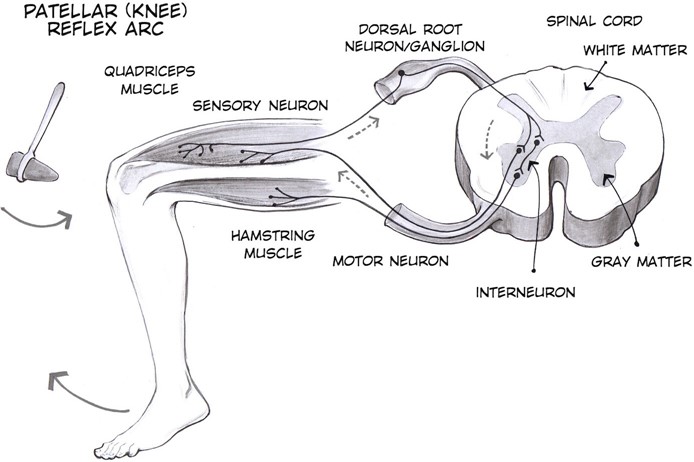
Choice D Reason: Patellar reflexes are absent. This is because absent patellar reflexes are a sign of magnesium sulfate toxicity, which is a condition where the level of magnesium in the blood is too high, which can cause adverse effects on the neuromuscular and cardiovascular systems. Magnesium sulfate is a medication that is used to prevent or treat preterm labor, which is labor that occurs before 37 weeks of gestation. Magnesium sulfate works by relaxing the uterine muscles and inhibiting uterine contractions. However, magnesium sulfate can also affect other muscles and nerves in the body, and cause symptoms such as muscle weakness, respiratory depression, hypotension, or cardiac arrest.
Correct Answer is D
Explanation
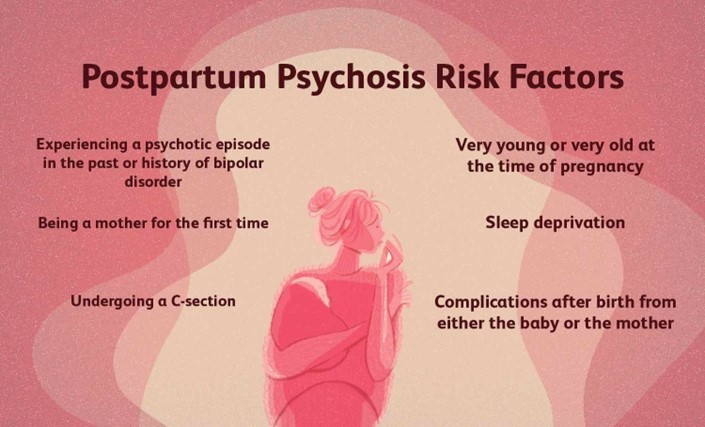
Choice A Reason: Maintain the client on strict bedrest. This is an inappropriate action that may worsen the client's condition and increase her isolation and depression. Postpartum psychosis requires prompt psychiatric treatment with medication and psychotherapy, not bedrest.
Choice B Reason: Carefully monitor intake and output. This is an irrelevant action that has no direct relation to postpartum psychosis or its management. Monitoring intake and output may be indicated for other postpartum complications such as hemorrhage, infection, or preeclampsia.
Choice C Reason: Restrict visitation of the client's partner. This is an unnecessary action that may deprive the client of social support and emotional comfort. The partner may be an important source of help and information for the client and the health care team. The partner should be involved in the client's care and education, unless there are signs of abuse or violence.
Choice D Reason: Closely supervise all infant care and interaction. This is because postpartum psychosis is a severe mental disorder that occurs in some women after childbirth, which can cause delusions, hallucinations, paranoia, mood swings, confusion, and suicidal or homicidal thoughts. Postpartum psychosis can pose a danger to both the mother and the infant, as the mother may harm herself or the infant due to distorted perceptions or impulses. The nurse should closely supervise all infant care and interaction to ensure safety and prevent injury.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today