The nurse is caring for an older client with that is exhibiting signs of confusion. Which intervention should the nurse implement?
Offer water to the client hourly.
Reduce dairy product intake.
Increase daily sodium intake.
Review the intake and output record.
The Correct Answer is D
Choice A
Offering water to the client hourly is not appropriate. While staying hydrated is important for overall health, offering water hourly might not be necessary unless there is a specific indication of dehydration. However, monitoring the client's fluid intake and output is a good approach.
Choice B
Reducing dairy product intake is not appropriate. Dairy product intake is not typically associated with sudden onset confusion. Reducing dairy product intake would not be the primary intervention for addressing confusion.
Choice C
Increasing daily sodium intake is not appropriate. Increasing sodium intake is unlikely to be the appropriate intervention for confusion unless there is a specific medical reason for it. Moreover, excessive sodium intake can have negative health consequences.
Choice D
Reviewing the intake and output record is appropriate. Confusion in an older client can be caused by various factors, including medical conditions, medication side effects, dehydration, and electrolyte imbalances. Reviewing the intake and output record (option D) is a reasonable intervention to gather more information about the client's fluid balance and hydration status. This can help the nurse assess whether the confusion might be related to dehydration or electrolyte imbalances.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A
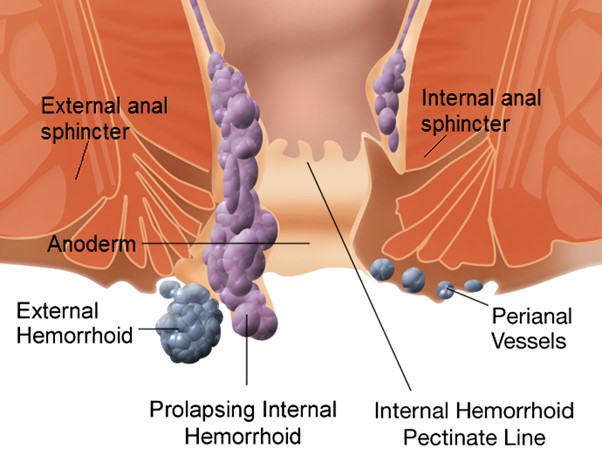
Explain the benefits of a high fibre diet is not correct response. While a high fibre diet can indeed be beneficial for individuals with haemorrhoids by promoting regular bowel movements and reducing strain during defecation, the immediate concern here is addressing the client's understanding about avoiding nuts and seeds. This information could be provided as a follow-up after confirming the client's understanding in response to option B.
Choice B
Confirm that these foods should be avoided is the correct response. In this situation, the nurse's first response should be to confirm the client's understanding and provide accurate information about the need to avoid certain foods. Nuts and seeds can be challenging to digest and may lead to irritation and inflammation in individuals with haemorrhoids. Confirming the client's understanding and providing guidance aligns with the nurse's role in patient education and care.
Choice C
Encourage soft foods such as yogurt is not the correct response. Encouraging soft foods like yogurt is a reasonable suggestion for someone with haemorrhoids, as soft foods are generally easier to digest and less likely to cause irritation. However, the client's statement was specifically about avoiding nuts and seeds. While this choice might be relevant, it doesn't directly address the client's statement.
Choice D
Suggest that the client also avoid fruit skins is not the correct response. This option is not directly related to the client's concern about nuts and seeds. Fruit skins generally contain dietary fibre, which can be beneficial for maintaining regular bowel movements. While some individuals might find that certain fruits with tough skins could exacerbate their haemorrhoid symptoms, this advice might be better suited for a separate discussion about dietary choices rather than as a direct response to the client's statement.
Correct Answer is ["B","D","E"]
Explanation
Choice A
Pickles, blackberries, seeds are not appropriate. None of these foods are particularly high in calcium. Pickles and blackberries are not significant sources of calcium, and while some seeds contain calcium, they are not among the best sources.
Choice B
Buttermilk, spinach, milk: These foods are good sources of dietary calcium is appropriate. Milk and buttermilk are commonly consumed dairy products that contain calcium. Spinach, while not as high in calcium as dairy products, still contributes to calcium intake.
Choice C
Pickled olives, spam, nuts are not appropriate. These foods are not known for being high in calcium. Additionally, some foods like pickled olives and spam may have high sodium content, which can affect calcium balance.
Choice D
Fresh meats, fresh turkey, fresh chicken is appropriate. Fresh meats, such as turkey and chicken, provide some calcium, although not as much as dairy products. They also contribute to overall nutritional intake.
Choice E
Cheese spread, processed cheese, cheese is appropriate. Dairy products like cheese, especially processed cheese and cheese spread, are good sources of calcium. They can be effective in increasing calcium intake to address hypocalcaemia.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today