The nurse is caring for a patient diagnosed with hypothyroidism. When assessing this patient, what sign or symptom would the nurse expect?
Flushed skin
Palpitations
Bulging eyes
Fatigue
The Correct Answer is D
A. Flushed skin: Flushed or warm skin is more characteristic of hyperthyroidism, where there is an excess of thyroid hormones.
B. Palpitations: Palpitations or a rapid heartbeat are more characteristic of hyperthyroidism, where there is an excess of thyroid hormones.
C. Bulging eyes: Bulging or protruding eyes, known as exophthalmos, is a characteristic sign of Graves' disease, which is a specific type of hyperthyroidism.
D. Fatigue: This is correct. Fatigue is a common symptom of hypothyroidism, reflecting the overall slowing down of the body's processes.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["C","E"]
Explanation
A. Asthma:
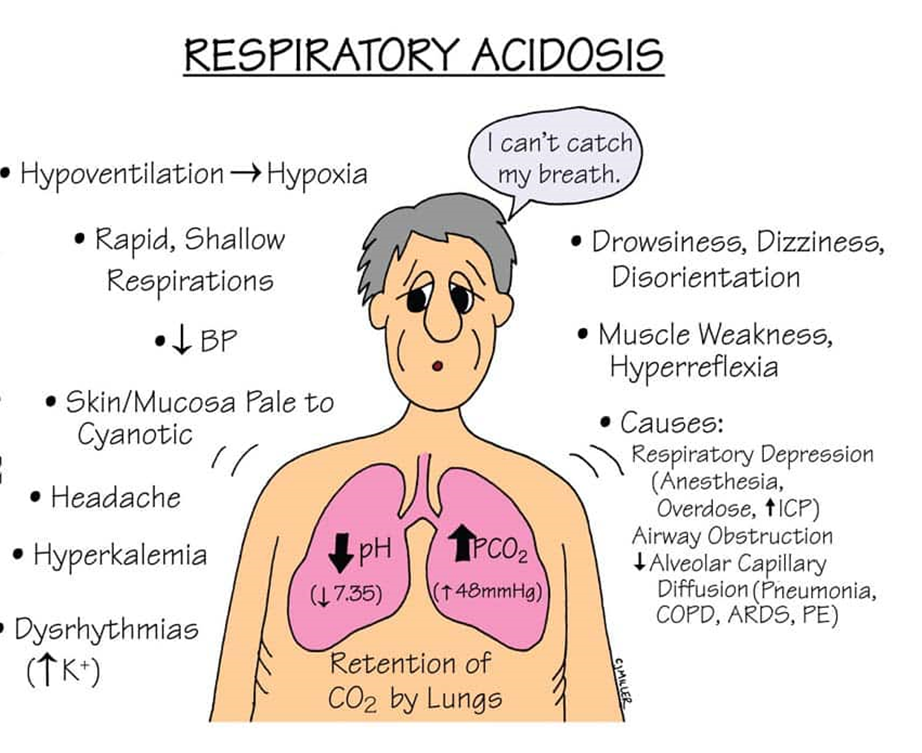
Explanation: Asthma is associated with respiratory alkalosis, not respiratory acidosis. In asthma, there is often hyperventilation leading to a decrease in carbon dioxide levels.
B. Hyperventilation:
Explanation: Correct. Hyperventilation can cause respiratory alkalosis, not respiratory acidosis. It leads to a decrease in carbon dioxide levels.
C. Chronic obstructive pulmonary disease (COPD):
Explanation: Correct. Conditions like COPD can lead to respiratory acidosis. In COPD, there is impaired ventilation, leading to an accumulation of carbon dioxide.
D. Renal insufficiency:
Explanation: Renal insufficiency is not a direct cause of respiratory acidosis. Respiratory acidosis is primarily related to respiratory system dysfunction.
E. Pneumonia:
Explanation: Correct. Pneumonia can cause respiratory acidosis. In pneumonia, there may be difficulty in eliminating carbon dioxide due to impaired gas exchange.
Correct Answer is D
Explanation
A. Respiratory acidosis:
This occurs when there is inadequate ventilation, leading to an accumulation of carbon dioxide (CO2) in the blood. In the context of a nasogastric tube attached to low suction, respiratory acidosis is not the primary concern. It is more associated with conditions like respiratory depression or lung diseases.
B. Metabolic acidosis:
Metabolic acidosis results from an excess of acid or a loss of bicarbonate. It is not the typical outcome of a nasogastric tube attached to low suction. Conditions like diarrhea or renal failure are more commonly associated with metabolic acidosis.
C. Respiratory alkalosis:
Respiratory alkalosis occurs when there is excessive loss of carbon dioxide from the body, often due to hyperventilation. This is not a typical consequence of a nasogastric tube attached to low suction.
D. Metabolic alkalosis:
Metabolic alkalosis is characterized by an excess of bicarbonate or a loss of acid. In the given context, with the nasogastric tube attached to low suction, there is a potential loss of gastric acid, contributing to metabolic alkalosis.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today