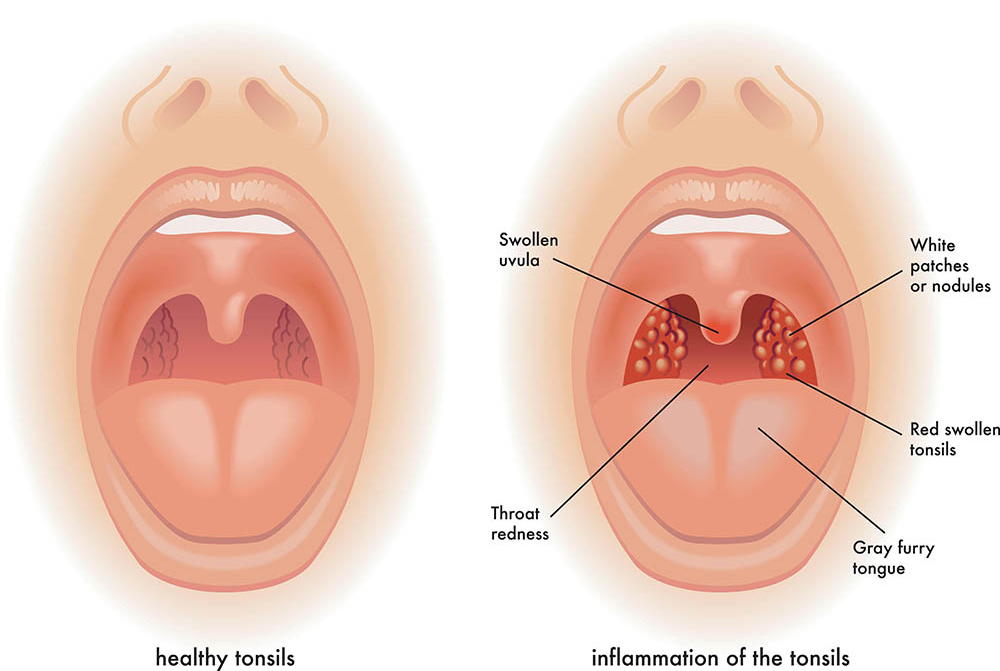
The nurse is assessing the tonsils of an adult client. The nurse notices that the tonsils are involuted, granular in appearance, and has deep crypts. The nurse recognizes that which of the following is the correct response to these findings?
Continue with the assessment, looking for any other abnormal findings.
Refer the patient to a throat specialist.
No response is needed; this appearance is normal for the tonsils.
Obtain a throat culture on the patient for possible streptococcal (strep) infection.
The Correct Answer is A
A. Continue with the assessment, looking for any other abnormal findings: This is the correct response. Tonsils in adults can have various appearances, and a granular appearance with deep crypts is within the range of normal. It's essential for the nurse to continue the assessment and observe for other signs or symptoms that might indicate an issue.
B. Refer the patient to a throat specialist: Referring the patient based solely on the appearance of the tonsils, especially if it's a normal variant, might be unnecessary and could cause undue concern for the patient. It's important to assess the patient comprehensively before considering a specialist referral.
C. No response is needed; this appearance is normal for the tonsils: This is the correct explanation. In adults, tonsils often appear granular with deep crypts, which is considered a normal variation. No further action is required regarding the tonsils.
D. Obtain a throat culture on the patient for possible streptococcal (strep) infection: Based on the description provided (involution, granular appearance, and deep crypts), there's no specific indication of a streptococcal infection. Conducting a throat culture should be based on the presence of specific symptoms and signs indicative of a streptococcal infection, such as sore throat, fever, and swollen tonsils with white patches, rather than just the appearance of the tonsils.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A. The best time to perform a BSE is 4 to 7 days after the first day of the menstrual period:
This statement is correct. Performing BSE a few days after the menstrual period ensures that the breasts are less likely to be swollen or tender, which can make it easier to detect any unusual changes.
B. If she suspects that she is pregnant, then the woman should not perform a BSE until her baby is born:
This statement is incorrect. Pregnant women can still perform breast self-examinations. In fact, it's important for pregnant women to be aware of any changes in their breasts.
C. The best time to perform BSE is in the middle of the menstrual cycle:
This statement is not as accurate as the first choice. While it's true that performing BSE a few days after the menstrual period can be easier due to reduced breast tenderness, it doesn't necessarily mean the middle of the menstrual cycle for every woman. The timing can vary based on an individual's menstrual cycle.
D. The woman needs to perform BSE only bimonthly unless she has fibrocystic breast tissue:
This statement is incorrect. Regular monthly breast self-examinations are recommended for all women, regardless of whether they have fibrocystic breast tissue or not. Detecting changes early is crucial for breast health.
Correct Answer is ["C","D"]
Explanation
A. Increased temperature: Fluid overload typically doesn't cause an increased temperature. Infections or other inflammatory processes are more likely causes of elevated body temperature.
B. Increased hematocrit: Fluid overload usually results in dilution of blood components, leading to a decreased hematocrit (lower concentration of red blood cells in the blood). An increased hematocrit is not a typical finding in fluid overload.
C. Blood pressure 180/100: Elevated blood pressure can be associated with fluid overload, especially if the overload is chronic. This is a correct assessment finding that requires intervention and monitoring.
D. Respiratory rate 32: An increased respiratory rate can be a sign of respiratory distress, which may occur in severe cases of fluid overload, especially if it leads to pulmonary edema. This is a correct assessment finding that requires intervention and further evaluation.
E. Heart rate 120 bpm: An increased heart rate can be a compensatory mechanism in response to fluid overload, especially if the heart is trying to maintain cardiac output. However, this heart rate alone is not specific enough to confirm fluid overload. Other signs and symptoms, such as edema, increased blood pressure, and respiratory distress, are more indicative of fluid overload.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today