The nurse is assessing a patient's postoperative wound and finds it has separated from the suture line with extrusion of the intestine through the opening. How does the nurse document this finding?
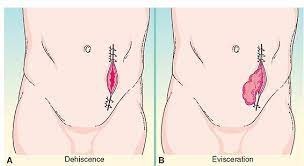
Wound evisceration
Wound dehiscence
Wound infection
Wound tunneling
The Correct Answer is A
Wound evisceration refers to the protrusion of internal organs or tissues through an open wound. In this case, with the separation of the wound and extrusion of the intestine through the opening, it is a clear indication of wound evisceration. It is a surgical emergency that requires immediate medical attention.
Wound dehiscence, on the other hand, refers to the separation or opening of a previously closed surgical incision or wound. It does not involve the extrusion of internal organs or tissues.
Wound infection refers to the presence of infectious microorganisms in the wound, leading to inflammation and other signs of infection.
Wound tunneling refers to the formation of narrow channels or tunnels within the wound, often caused by improper wound healing or infection.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
According to the given information, Aydan's insulin lispro (Humalog) dosage is 1 unit per 50 grams of carbohydrates eaten. As Aydan has just consumed 150 grams of carbs for lunch, we can calculate the insulin dose as follows:
Insulin dose = Carbohydrates eaten / Insulin-to-carbohydrate ratio Insulin dose = 150 grams / 50 grams/unit
Insulin dose = 3 units
Therefore, the nurse should prepare to administer 3 units of Aydan's prescribed rapid-acting insulin (Insulin lispro) to cover the carbohydrates he consumed for lunch. The long-acting insulin (Glargine) is typically given at bedtime to provide a basal insulin level and is not directly related to meal coverage.
Correct Answer is A
Explanation
Acute renal failure is characterized by a sudden decline in kidney function, resulting in the inability of the kidneys to adequately filter waste products and maintain fluid and electrolyte balance. Monitoring urine output is essential in assessing kidney function and determining the severity of renal failure. A decrease in urine output or anuria may indicate worsening renal function and the need for immediate interventions.
Assessing electrolyte levels, such as sodium, potassium, calcium, and phosphorus, is crucial because renal failure can disrupt the balance of these electrolytes in the body. Imbalances can lead to complications such as electrolyte abnormalities, cardiac dysrhythmias, and neuromuscular disturbances. Prompt identification and management of electrolyte imbalances are essential in preventing further complications and supporting optimal patient outcomes.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today