The nurse is assessing a first day postpartum client. Which finding is most indicative of a postpartum infection?
White Blood Cell (WBC. Reference Range: 5000-10,000/mm^3 (5-10 x 10^9/L)
Moderate amount of foul-smelling lochia.
Blood pressure of 122/74 mm Hg
Oral temperature of 100.2°F (37.9°C..
White blood cell count of 19,000/mm^3 (19 x 10^9/L)
The Correct Answer is A
Choice B reason: Blood pressure of 122/74 mm Hg is within the normal range for a postpartum client and does not indicate an infection. However, the nurse should monitor for signs of preeclampsia or eclampsia, such as hypertension, proteinuria, headache, blurred vision, and seizures.
Choice C reason: Oral temperature of 100.2°F (37.9°C. is slightly elevated, but not necessarily indicative of an infection. A mild fever may occur within the first 24 hours after delivery due to dehydration or hormonal changes. However, if the fever persists or increases, the nurse should suspect an infection and notify the healthcare provider.
Choice D reason: White blood cell count of 19,000/mm^3 (19 x 10^9/L) is higher than the normal range, but not necessarily indicative of an infection. A leukocytosis or increased WBC count may occur as a normal response to stress or trauma during delivery. However, if the WBC count remains elevated or increases further, the nurse should suspect an infection and notify the healthcare provider.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
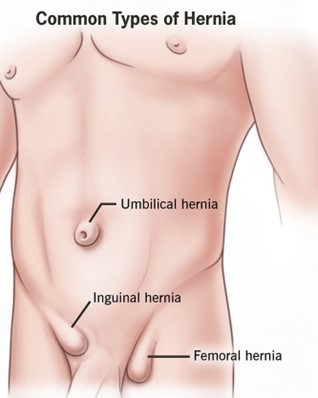
Choice A: This hernia is a normal variation that resolves without treatment is a correct explanation for the nurse to provide, as this refers to an umbilical hernia, which is a common and harmless condition in infants that usually disappears by age 2. Therefore, this is the correct choice.
Choice B: An abdominal binder can be worn daily to reduce the protrusion is not an appropriate explanation for the nurse to provide, as this is not an effective or recommended method to treat a hernia. This is a distractor choice.
Choice C: Restrictive clothing will be adequate to help the hernia go away is not a relevant explanation for the nurse to provide, as this does not affect the hernia or its resolution. This is another distractor choice.
Choice D: The quarter should be secured with an elastic bandage wrap is not a sensible explanation for the nurse to provide, as this is a folk remedy that has no scientific basis and can cause skin irritation and infection. This is another distractor choice.
Correct Answer is D
Explanation
Choice D is correct because frequent exposure to sunlight is the most significant environmental factor when planning care for a client with osteomalacia. Osteomalacia is a condition in which the bones become soft and weak due to inadequate mineralization, often caused by vitamin D deficiency. Vitamin D is essential for calcium absorption and bone health, and it can be synthesized by the skin when exposed to sunlight. The nurse should encourage the client to get at least 15 minutes of sunlight per day or take vitamin D supplements as prescribed.
Choice A is incorrect because quiet, calm surroundings are not a specific environmental factor for a client with osteomalacia. Quiet, calm surroundings may help reduce stress and promote relaxation, but they do not affect bone mineralization or vitamin D synthesis.
Choice B is incorrect because stimulating sounds and activity are not a specific environmental factor for a client with osteomalacia. Stimulating sounds and activity may help improve mood and cognition, but they do not affect bone mineralization or vitamin D synthesis.
Choice C is incorrect because cool, moist air is not a specific environmental factor for a client with osteomalacia. Cool, moist air may help relieve respiratory symptoms or allergies, but it does not affect bone mineralization or vitamin D synthesis.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today