Which assessment should the home health nurse include during a routine home visit for a client who was discharged home with a suprapubic catheter?
Observe insertion site.
Palpate flank area.
Measure abdominal girth.
Assess perineal area.
The Correct Answer is A
Choice A: Observing insertion site is an essential assessment for a client who has a suprapubic catheter. The insertion site is located in the lower abdomen, where urine drains from an opening in the bladder through a catheter into a drainage bag. The nurse should inspect the site for signs of infection, inflammation, bleeding, or leakage. The nurse should also clean the site with soap and water and apply a sterile dressing as needed.
Choice B: Palpating flank area is not a relevant assessment for a client who has a suprapubic catheter. The flank area is located on the sides of the back, where the kidneys are located. Palpating the flank area can detect tenderness or pain that may indicate kidney infection or stones, but it does not provide information about the suprapubic catheter or its function.
Choice C: Measuring abdominal girth is not a relevant assessment for a client who has a suprapubic catheter. The abdominal girth is the circumference of the abdomen at the level of the umbilicus. Measuring abdominal girth can detect changes in fluid balance, ascites, or bowel obstruction, but it does not provide information about the suprapubic catheter or its function.
Choice D: Assessing perineal area is not a relevant assessment for a client who has a suprapubic catheter. The perineal area is located between the anus and the genitals. Assessing perineal area can detect signs of infection, irritation, or injury in the genital or anal regions, but it does not provide information about the suprapubic catheter or its function.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason: Support stockings may help with peripheral edema, but they are not the priority intervention for this client. The client's low serum albumin level indicates malnutrition and increased risk of infection and poor wound healing.
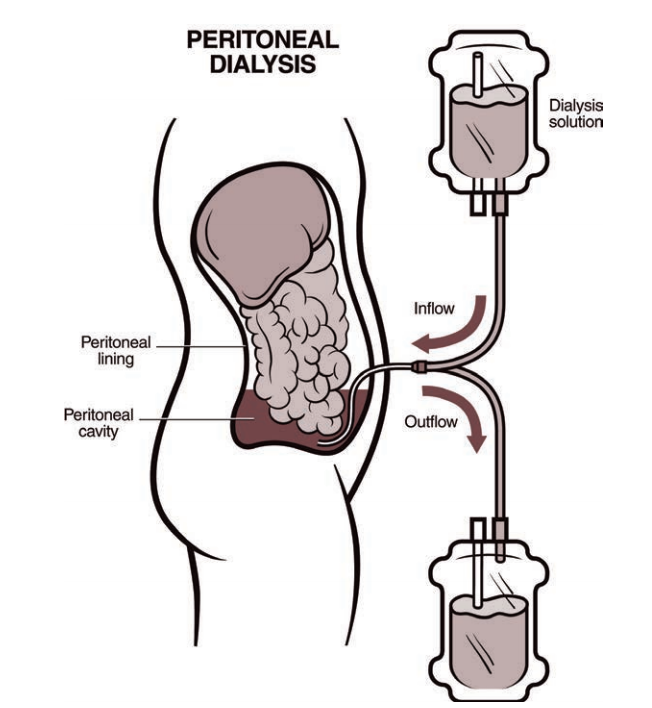
Choice C reason: Evaluating patency of the AV graft is not the priority intervention for this client because the client is receiving peritoneal dialysis, not hemodialysis. The AV graft may be used in the future if peritoneal dialysis fails, but it is not an immediate concern.
Choice D reason: Instructing the client to follow fluid restriction amounts is important for peritoneal dialysis patients, but it is not the priority intervention for this client. The client's low serum albumin level indicates that fluid restriction alone is not sufficient to manage fluid balance and prevent edema.
Correct Answer is C
Explanation
Choice A: An adolescent with multiple contusions due to a fall that occurred 2 days ago is not a client that the charge nurse should assign to the RN, as this is a stable and low-acuity client who can be safely cared for by the PN. This is a distractor choice.
Choice B: A 75-year-old client with renal calculi who requires urine straining is not a client that the charge nurse should assign to the RN, as this is a routine and non-complex task that can be performed by the PN. This is another distractor choice.
Choice C: A 30-year-old depressed client who admits to suicide ideation is a client that the charge nurse should assign to the RN, as this is an unstable and high-risk client who requires close monitoring, assessment, and intervention by the RN. Therefore, this is the correct choice.
Choice D: A 64-year-old client who had a total hip replacement the previous day is not a client that the charge nurse should assign to the RN, as this is a postoperative and moderate-acuity client who can be managed by the PN under the supervision of the RN. This is another distractor choice.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today