Prior to giving digoxin, the practical nurse (PN) assesses that a 2-month-old infant's heart rate is 120 beats/minute. Based on this finding, which action should the PN take?
Hold the medication and recheck the heart rate in l hour.
Administer the medication and document the heart rate.
Administer the medication and alert the charge nurse.
Hold the medication and document cardiac assessment.
The Correct Answer is B
Digoxin is a medication used to treat various heart conditions, such as abnormal heart rhythms and heart failure. It works by improving the strength and efficiency of the heart, or by controlling the rate and rhythm of the heartbeat.
One of the important things to monitor when giving digoxin to an infant is the pulse rate. Digoxin can lower the heart rate, which can be dangerous if it becomes too slow. Therefore, the pulse rate should be checked for one full minute before administering digoxin, and the medication should be held if the pulse rate is below 90 beats per minute (bpm) for an infant.
In this case, the infant’s heart rate is 120 bpm, which is within the normal range for a 2-month-old. Therefore, the correct action for the PN to take is to administer the medication and document the heart rate. This is option b in the list of choices. Option a is incorrect because there is no need to hold the medication or recheck the heart rate in one hour. Option c is incorrect because there is no need to alert the charge nurse unless there is a problem with the infant’s condition or the medication. Option d is incorrect because holding the medication and documenting cardiac assessment is not appropriate for a normal heart rate.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
The correct answer is choice C - IV infusion site is infiltrated. Choice A rationale:
The client reports feeling nauseous. While this symptom should be monitored, it is not the most crucial finding to report for a client in Addison's crisis. Nausea can be a common symptom during various medical conditions and may not warrant immediate action.
Choice B rationale:
Has not voided in four hours. While monitoring urine output is important, it may not be the most critical finding in Addison's crisis. Other symptoms like electrolyte imbalances and
circulatory collapse is more concerning in this scenario.
Choice C rationale:
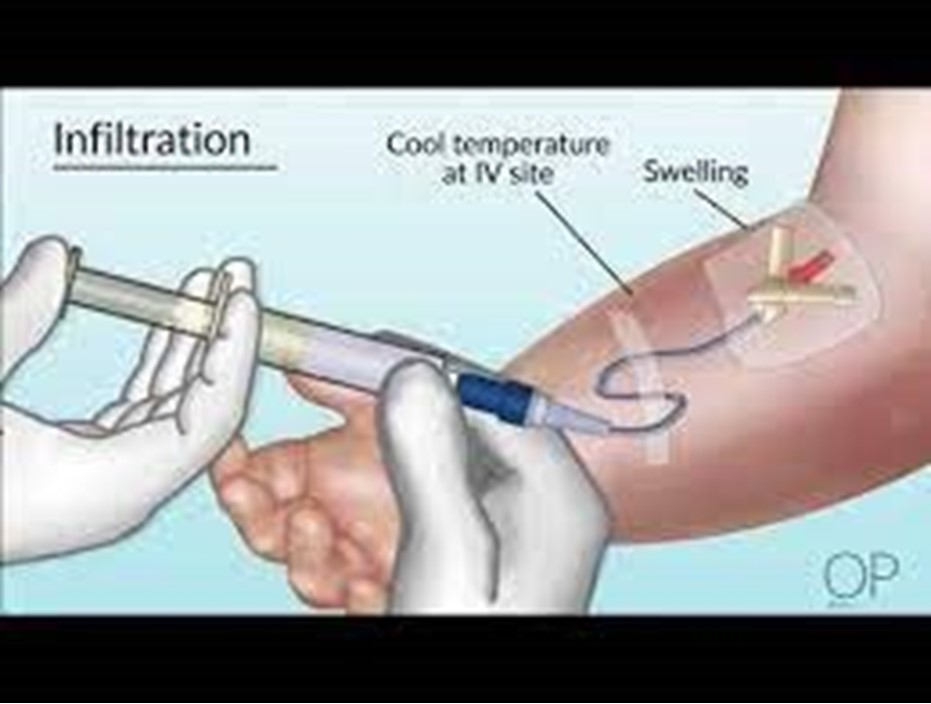
IV infusion site is infiltrated. In Addison's crisis, the client's condition may be precarious, and any complications with IV therapy could worsen the situation. It is essential to report this finding promptly to prevent further complications.
Choice D rationale:
A serum glucose level of 85 mg/dL. While monitoring glucose levels is essential in many situations, a glucose level of 85 mg/dL is within the reference range, which means it is not the most critical finding in Addison's crisis.
Correct Answer is B
Explanation
This is the action that the PN should emphasize for the client to take before self-administration of the nasal spray because it clears the nasal passages of mucus and debris and allows for better absorption of the medication. The PN should also instruct the client to shake the botle well, tilt the head slightly forward, insert the nozzle into one nostril, close the other nostril with a finger, and press the pump while inhaling gently.

Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today