A client who is one day postpartum reports to the nurse that her baby cannot latch onto the breast. The nurse observes that the client's nipples are inverted. Which action should the nurse implement?
Offer supplemental formula feedings.
Teach about the use of a breast pump.
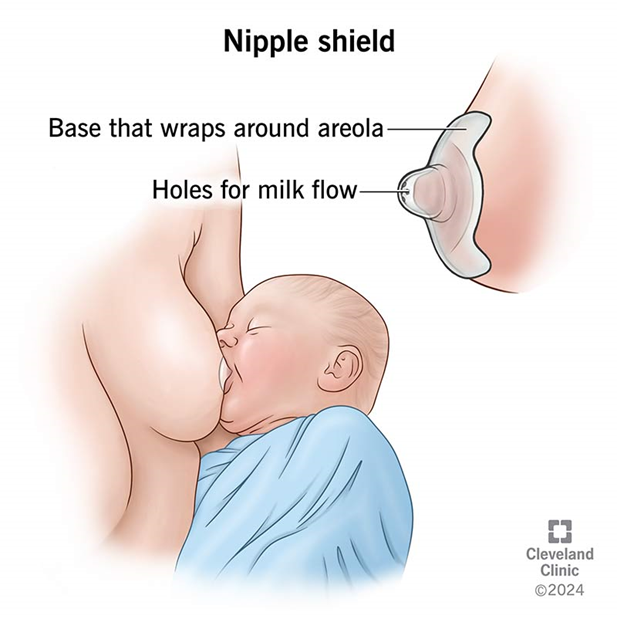
Recommend using a breast shield.
Encourage the use of ice on the areola.
The Correct Answer is C
The correct answer is c. Recommend using a breast shield.
Choice A reason: Offering supplemental formula feedings is not the first-line action for inverted nipples as it does not address the issue and may lead to nipple confusion, potentially complicating future breastfeeding attempts.
Choice B reason: Teaching about the use of a breast pump is beneficial for milk expression but does not directly assist with the immediate concern of latching issues due to inverted nipples.
Choice C reason: Using a breast shield can be helpful for mothers with inverted nipples. It can temporarily draw out the nipple, allowing the baby to latch on more easily. This tool acts as a bridge between the breast and the baby's mouth, facilitating breastfeeding while the mother works on long-term solutions for her inverted nipples.
Choice D reason: Encouraging the use of ice on the areola may temporarily stiffen the nipple, but it is not a recommended practice for addressing inverted nipples as it can cause discomfort and may not be effective in promoting a successful latch.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A rationale:
Referring the client to a social worker for support therapy may be premature at this stage. The client's initial reaction may be due to fear or anxiety about the diagnosis and self-administration of insulin. Pushing the client into therapy without assessing their readiness may not be appropriate.
Choice B rationale:
Encouraging the client to implement relaxation techniques assumes that the client is open to learning and just needs help with anxiety management. However, the client's refusal to have the nurse in the room suggests that they are not currently receptive to teaching. It's important to address the client's emotional state first.
Choice C rationale:
Leaving the client's room and returning later in the day is the most appropriate initial action. The client's loud refusal indicates a need for privacy and emotional space. By respecting the client's wishes and revisiting the teaching later, the nurse can establish trust and build a better rapport.
Choice D rationale:
Explaining that insulin is a life-saving drug is informative but may not be effective in this situation, as the client has already requested the nurse to leave the room. Providing information about the importance of insulin should come after establishing a therapeutic nurse-client relationship.
Correct Answer is A
Explanation
The correct answer is **a. Report the finding to the healthcare provider.**
Choice A rationale:
The nurse should report the finding of the client's response to a painful stimulus to the healthcare provider. This response, known as a decorticate posturing, is an abnormal motor response that indicates a severe brain injury or dysfunction. It is a sign of impaired consciousness and requires immediate medical attention and intervention.
Choice B rationale:
While documenting the client's response to pain is important, the primary action the nurse should take is to report the finding to the healthcare provider. Decorticate posturing is a neurological emergency that requires prompt medical evaluation and treatment.
Choice C rationale:
Initiating seizure precautions is not the appropriate action in this case. Decorticate posturing is not a seizure, but rather an abnormal motor response indicating a severe brain injury or dysfunction. Seizure precautions would not be the appropriate intervention.
Choice D rationale:
Administering a prescribed PRN analgesic is not the appropriate action in this case. Decorticate posturing is a neurological emergency that requires immediate medical attention, not just pain management. Administering an analgesic would not address the underlying neurological issue.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today