The nurse is educating a client about essential hypertension prevention. Which information should the nurse provide? (Select all that apply)
Alcohol consumption will not produce vascular changes.
Weight management is promoted by taking daily walks for thirty minutes.
Salt substitutes can help with maintaining a healthy diet.
Blood pressure readings should be taken at noontime.
Sodium intake can be regulated by rinsing canned foods in water.
Uncontrolled hypertension can lead to renal damage.
Correct Answer : B,C,E,F
Choice B reason: weight management is an important factor in preventing and controlling hypertension. Taking daily walks for thirty minutes can help reduce weight and lower blood pressure.
Choice C reason: salt substitutes can help with maintaining a healthy diet by reducing sodium intake. Sodium intake is associated with increased blood pressure and should be limited to less than 2,300 mg per day.
Choice E reason: sodium intake can be regulated by rinsing canned foods in water. Canned foods often contain high amounts of sodium as a preservative and rinsing them can remove some of the excess sodium.
Choice F reason: uncontrolled hypertension can lead to renal damage. Hypertension can cause damage to the blood vessels and impair the function of the kidneys, leading to chronic kidney disease or failure.
Choice A reason: alcohol consumption can produce vascular changes that increase blood pressure. Alcohol intake should be limited to no more than one drink per day for women and two drinks per day for men.
Choice D reason: blood pressure readings should not be taken at noontime. Blood pressure readings should be taken at the same time each day, preferably in the morning before breakfast or in the evening before dinner.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","C","D"]
Explanation
Choice A reason: Taking metformin with the morning and evening meal is a correct statement for the nurse to include, as this can improve the absorption and effectiveness of metformin and reduce the risk of gastrointestinal side effects. Therefore, this is a correct choice.
Choice B reason: Using sliding scale insulin for frequent blood glucose elevations is not a correct statement for the nurse to include, as this is not recommended for clients with type 2 DM who are taking metformin. This can cause hypoglycemia and complicate the management of blood glucose levels. This is an incorrect choice.
Choice C reason: Recognizing signs and symptoms of hypoglycemia is a correct statement for the nurse to include, as this can help the client identify and treat low blood glucose levels, which can occur with metformin use or other factors such as exercise, fasting, or alcohol intake. Therefore, this is another correct choice.
Choice D reason: Reporting persistent polyuria to the health care provider is a correct statement for the nurse to include, as this can indicate poor glycemic control or a complication of DM such as diabetic ketoacidosis or nephropathy. Therefore, this is another correct choice.
Choice E reason: Taking an additional dose for signs of hyperglycemia is not a correct statement for the nurse to include, as this can cause overdose or toxicity of metformin, which can lead to lactic acidosis and renal failure. This is another incorrect choice.
Correct Answer is B
Explanation
Choice A reason: Support stockings may help with peripheral edema, but they are not the priority intervention for this client. The client's low serum albumin level indicates malnutrition and increased risk of infection and poor wound healing.
Choice B reason: This is the correct answer because the client needs adequate protein intake to maintain serum albumin levels and prevent further complications. Complete proteins contain all nine essential amino acids that the body cannot synthesize and are found in animal sources such as meat, eggs, and dairy products.
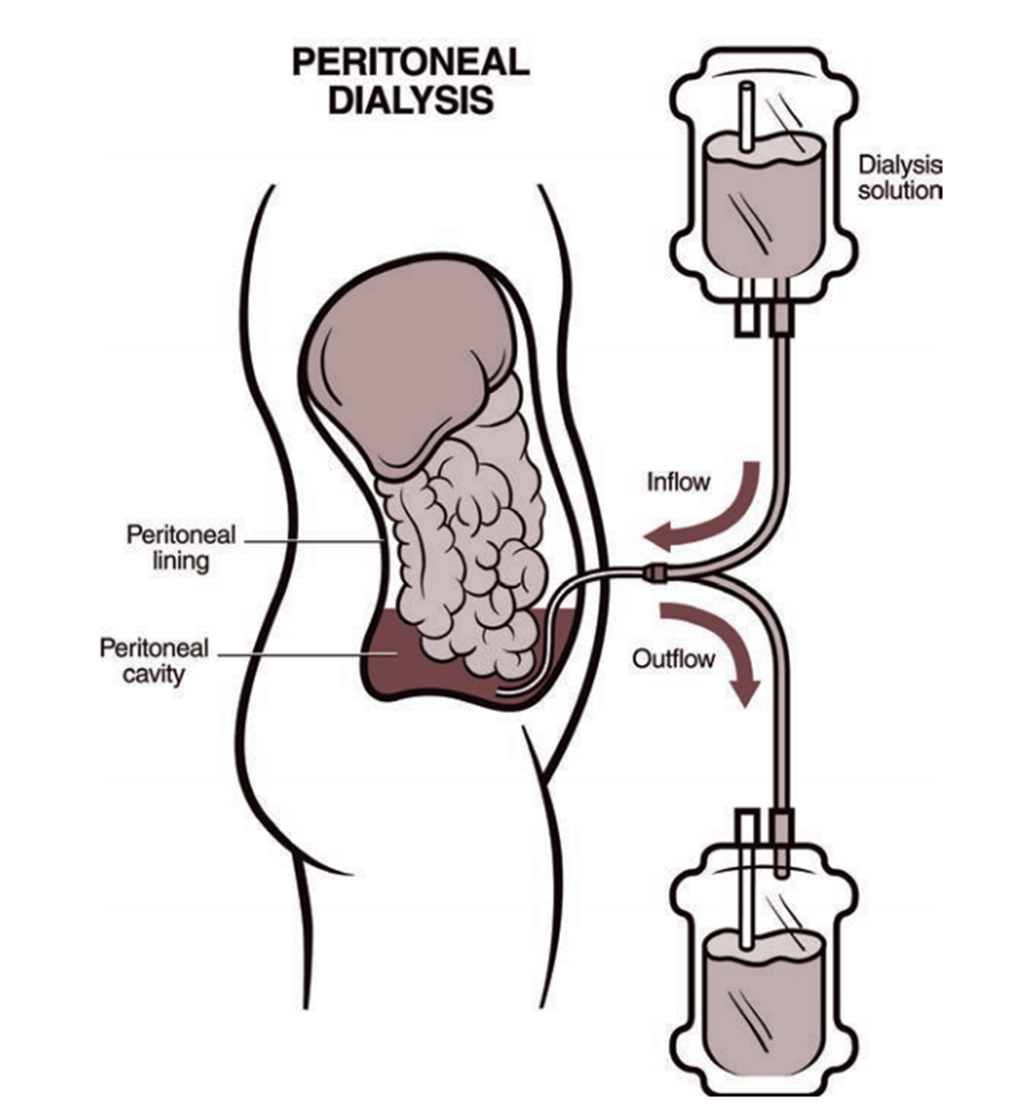
Choice C reason: Evaluating patency of the AV graft is not the priority intervention for this client because the client is receiving peritoneal dialysis, not hemodialysis. The AV graft may be used in the future if peritoneal dialysis fails, but it is not an immediate concern.
Choice D reason: Instructing the client to follow fluid restriction amounts is important for peritoneal dialysis patients, but it is not the priority intervention for this client. The client's low serum albumin level indicates that fluid restriction alone is not sufficient to manage fluid balance and prevent edema.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today