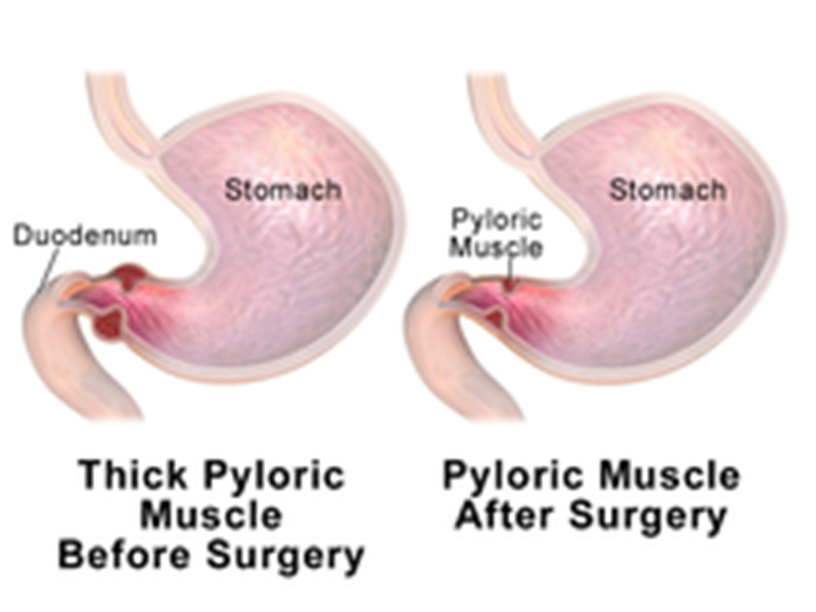
A 6-week-old infant with poor weight gain is scheduled for a pyloromyotomy. Which pre-operative nursing action has the highest priority?
Mark an outline of the "olive-shaped" mass in the right epigastric area.
Maintain a continuous infusion of IV fluids per prescription.
Monitor amount of intake and infant's response to feedings.
Instruct parents regarding care of the incisional area.
The Correct Answer is B
Choice A reason: Marking an outline of the "olive-shaped" mass in the right epigastric area is not a priority nursing action. The mass is caused by hypertrophy of the pyloric sphincter, which obstructs gastric emptying and causes projectile vomiting. The mass may not be palpable in all cases.
Choice B reason: This is the correct answer because maintaining a continuous infusion of IV fluids per prescription is essential to prevent dehydration and electrolyte imbalance in the infant. The infant may have significant fluid loss due to vomiting and poor intake.
Choice C reason: Monitoring amount of intake and infant's response to feedings is important, but not the highest priority. The infant may have difficulty feeding due to nausea, vomiting, and abdominal pain.
Choice D reason: Instructing parents regarding care of the incisional area is a post-operative nursing action, not a pre-operative one. The parents will need to learn how to keep the incision clean and dry, monitor for signs of infection, and administer pain medication as prescribed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: 18%. This is not the correct percentage, as it only accounts for one lower extremity. According to the rule of nines, each lower extremity accounts for 9% of body surface area on both anterior and posterior sides, so both lower extremities would account for 18% x 2 = 36%.
Choice B reason: 27%. This is not the correct percentage, as it only accounts for one and a half lower extremities. According to the rule of nines, each lower extremity accounts for 9% of body surface area on both anterior and posterior sides, so one and a half lower extremities would account for 9% x 3 = 27%.
Choice C reason: 36%. This is the correct percentage, as it accounts for both lower extremities. According to the rule of nines, each lower extremity accounts for 9% of body surface area on both anterior and posterior sides, so both lower extremities would account for 9% x 4 = 36%.
Choice D reason: 45%. This is not the correct percentage, as it accounts for more than both lower extremities. According to the rule of nines, each lower extremity accounts for 9% of body surface area on both anterior and posterior sides, so more than both lower extremities would account for more than 9% x 4 = 36%.
Correct Answer is ["A","B","D"]
Explanation
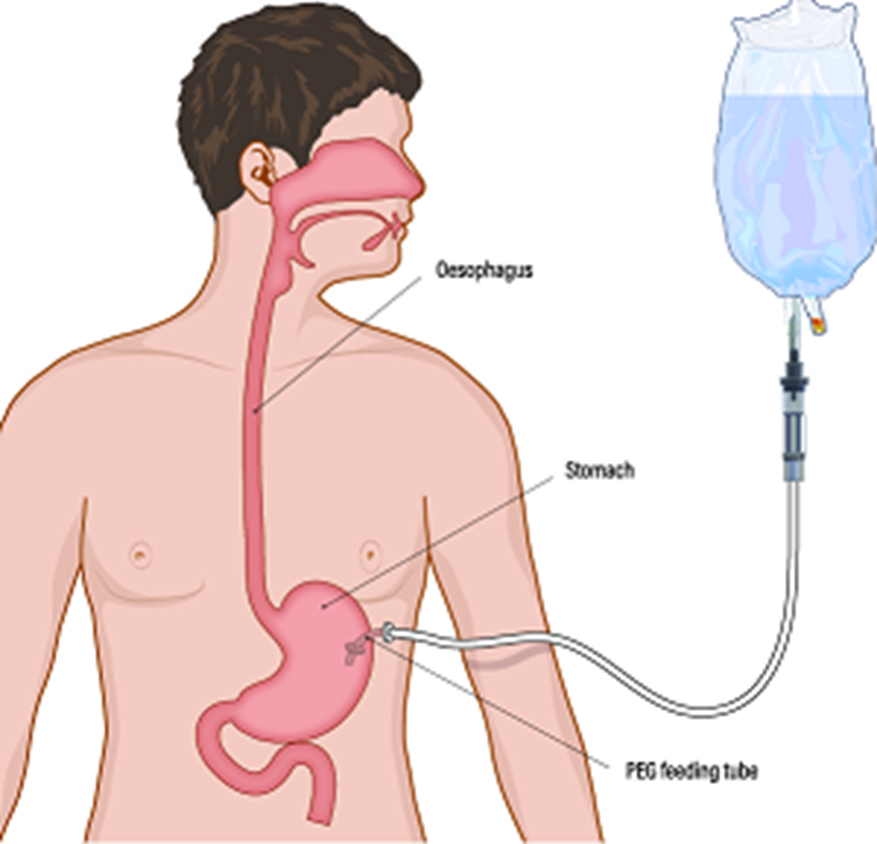
Choice A reason: This is a correct answer because flushing the tube with more water is important to prevent clogging and maintain hydration. The novice should flush the tube with at least 15 mL of water before and after each medication, and between medications if more than one is given.
Choice B reason: This is a correct answer because administering each medication separately is important to prevent interactions and ensure accurate dosing. The novice should not mix different medications in one syringe or container, but give them one at a time, followed by water flushes.
Choice C reason: This is not a correct answer because adding the liquid volumes when documenting fluid intake is not necessary. The liquid medications do not count as fluid intake, but as medication administration. The novice should document the type, dose, route, and time of each medication given, as well as any adverse effects or complications.
Choice D reason: This is a correct answer because confirming that the novice determined the amount of gastric residual is important to assess tolerance and prevent aspiration. The novice should aspirate the gastric contents with a syringe before giving any medication or feeding, and measure and document the volume. If the volume is more than 100 mL or the prescribed amount, the novice should hold the medication or feeding and notify the healthcare provider.
Choice E reason: This is not a correct answer because advising the novice to use the plunger when giving medications is not recommended. The novice should use gravity to deliver the medications through the tube, by holding the syringe upright and allowing the liquid to flow slowly. Using the plunger can cause too much pressure and damage the tube or cause discomfort to the client.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today