Three hours after birth, a newborn becomes jittery and tachypneic. What should the nurse do first?
Obtain a capillary glucose level.
Feed 30 mL of 10% dextrose in water.
Wrap tightly in a blanket.
Encourage the mother to breastfeed.
None
None
The Correct Answer is A
Choice A: Obtain a capillary glucose level. This is the first action that the nurse should do, as it can diagnose hypoglycemia, which is a low blood sugar level that can cause jitteriness and tachypnea in newborns. Hypoglycemia can be caused by maternal diabetes, prematurity, infection, or delayed feeding. The nurse should check the glucose level using a heel stick and a glucometer.
Choice B: Feed 30 mL of 10% dextrose in water. This is not the first action that the nurse should do, as it may not be appropriate for all newborns with jitteriness and tachypnea. Feeding 10% dextrose in water can raise the blood sugar level, but it may also cause rebound hypoglycemia or fluid overload. The nurse should feed only after confirming hypoglycemia and obtaining a healthcare provider's order.
Choice C: Wrap tightly in a blanket. This is not the first action that the nurse should do, as it may not address the underlying cause of jitteriness and tachypnea in newborns. Wrapping tightly in a blanket can prevent heat loss and conserve energy, but it may also impair breathing or circulation. The nurse should wrap only after ruling out other causes of jitteriness and tachypnea.
Choice D: Encourage the mother to breastfeed. This is not the first action that the nurse should do, as it may not be feasible or effective for all newborns with jitteriness and tachypnea. Breastfeeding can provide nutrition and bonding for newborns, but it may also be difficult or contraindicated for some newborns with respiratory distress or infection. The nurse should encourage breastfeeding only after assessing and stabilizing the newborn's condition.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
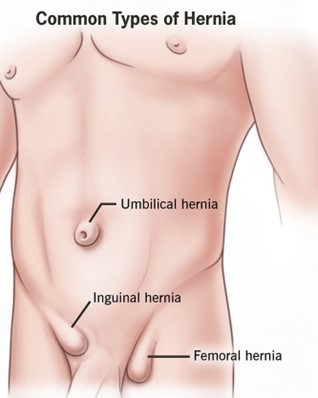
Choice A: This hernia is a normal variation that resolves without treatment is a correct explanation for the nurse to provide, as this refers to an umbilical hernia, which is a common and harmless condition in infants that usually disappears by age 2. Therefore, this is the correct choice.
Choice B: An abdominal binder can be worn daily to reduce the protrusion is not an appropriate explanation for the nurse to provide, as this is not an effective or recommended method to treat a hernia. This is a distractor choice.
Choice C: Restrictive clothing will be adequate to help the hernia go away is not a relevant explanation for the nurse to provide, as this does not affect the hernia or its resolution. This is another distractor choice.
Choice D: The quarter should be secured with an elastic bandage wrap is not a sensible explanation for the nurse to provide, as this is a folk remedy that has no scientific basis and can cause skin irritation and infection. This is another distractor choice.
Correct Answer is C
Explanation
Choice A: Straining all urine is not a relevant instruction for the nurse to provide, as this is not related to prostatitis. This is a distractor choice.
Choice B: Maintaining contact isolation is not a necessary instruction for the nurse to provide, as prostatitis is not a contagious condition. This is another distractor choice.
Choice C: Avoiding urinary catheterization is an important instruction for the nurse to provide, as this can introduce bacteria into the urinary tract and worsen the infection. Therefore, this is the correct choice.
Choice D: Restricting oral fluid intake is not an appropriate instruction for the nurse to provide, as this can lead to dehydration and reduced urine output, which can increase the risk of urinary stasis and infection. This is another distractor choice.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today