Days after surgical fixation of a fractured femur, a client suddenly reports chest pain and difficulty in breathing. The nurse suspects that the client had a pulmonary embolus. Which action should the nurse take first?
Notify the healthcare provider.
Prepare a continuous heparin infusion per protocol.
Provide supplemental oxygen.
Bring the emergency crash cart to the bedside.
The Correct Answer is C
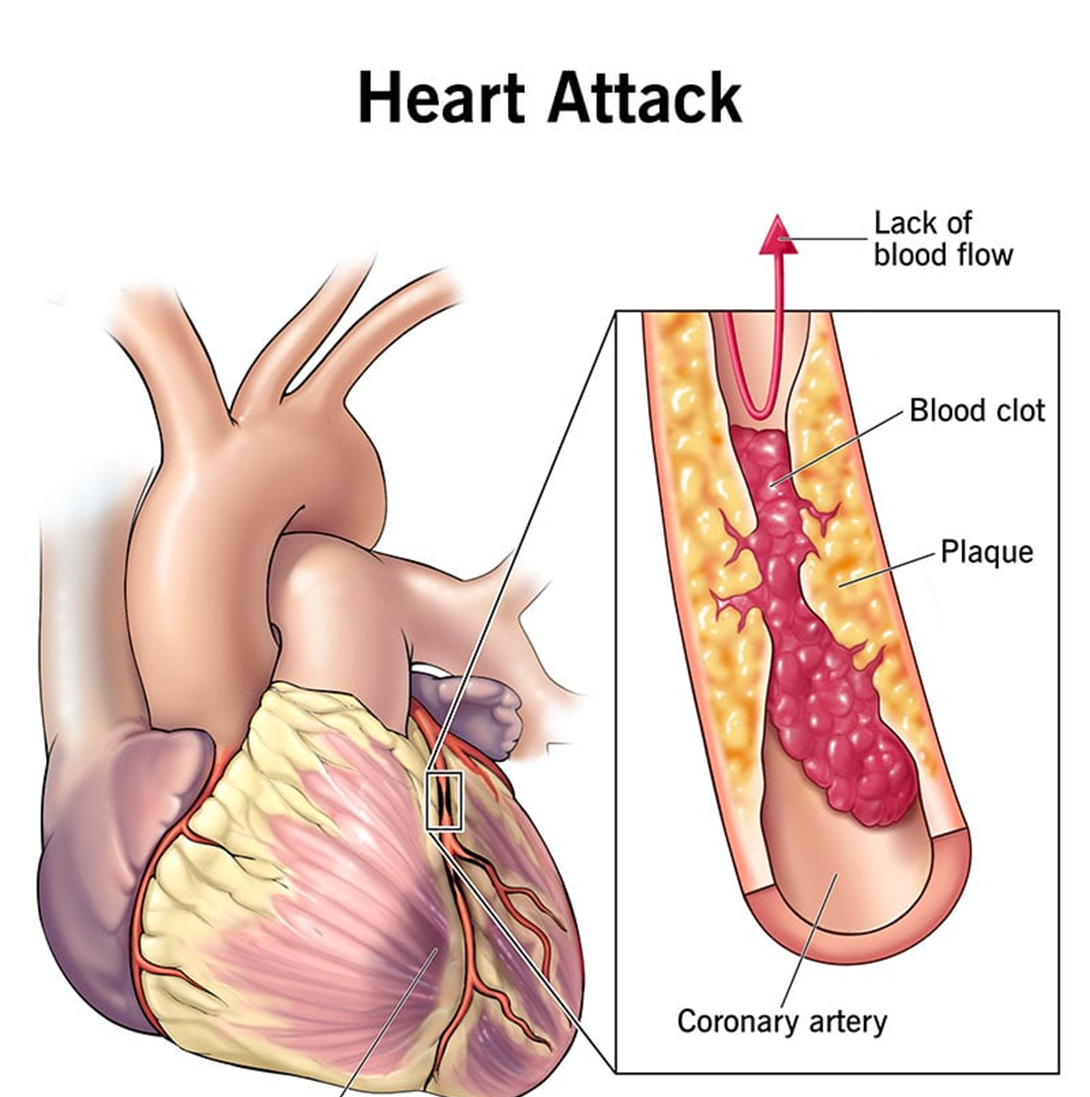
Choice C reason: providing supplemental oxygen is the first action that the nurse should take for a client who has a suspected pulmonary embolus. A pulmonary embolus is a life-threatening condition that occurs when a blood clot travels to the lungs and blocks the blood flow, causing hypoxia and respiratory distress. The nurse should administer oxygen to improve the client's oxygenation and prevent further complications.

Choice A reason: notifying the healthcare provider is not the first action that the nurse should take for a client who has a suspected pulmonary embolus. The nurse should notify the healthcare provider after providing supplemental oxygen and assessing the client's vital signs and symptoms.
Choice B reason: preparing a continuous heparin infusion per protocol is not the first action that the nurse should take for a client who has a suspected pulmonary embolus. Heparin is an anticoagulant that can prevent further clot formation and reduce the risk of recurrence, but it does not dissolve existing clots or improve oxygenation. The nurse should prepare a heparin infusion after obtaining a prescription from the healthcare provider and confirming the diagnosis with diagnostic tests.
Choice D reason: bringing the emergency crash cart to the bedside is not the first action that the nurse should take for a client who has a suspected pulmonary embolus. The emergency crash cart contains equipment and medications that can be used in case of cardiac arrest or other emergencies, but it does not address the immediate need of oxygenation. The nurse should bring the emergency crash cart to the bedside after providing supplemental oxygen and assessing the client's condition.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: This is the correct answer because ineffective coping related to denial is a likely problem for a client who had an MI 24 hours ago and wants to go home despite his condition. Denial is a defense mechanism that helps people avoid facing unpleasant or threatening realities, such as having a heart attack and needing hospitalization and treatment. The nurse should assess the client's coping skills and provide emotional support and education.
Choice B reason: Emotional conflict due to stress is not a specific problem for a client who had an MI 24 hours ago and wants to go home despite his condition. Emotional conflict is a state of having mixed or contradictory feelings about something or someone, such as family, work, or self. Stress is a response to any physical, psychological, or environmental demand that exceeds one's coping resources. The nurse should assess the client's sources of stress and conflict and help him manage them.
Choice C reason: Deficient knowledge of MI lifestyle changes is not a primary problem for a client who had an MI 24 hours ago and wants to go home despite his condition. Deficient knowledge is a state of lacking information or understanding about something, such as disease process, treatment options, or self-care measures. Lifestyle changes are modifications in one's habits or behaviors that promote health and well-being, such as diet, exercise, smoking cessation, or stress management. The nurse should assess the client's learning needs and readiness and provide appropriate education.
Choice D reason: Anxiety related to treatment plan is not an evident problem for a client who had an MI 24 hours ago and wants to go home despite his condition. Anxiety is a feeling of apprehension, worry, or fear that interferes with one's normal functioning or well-being. Treatment plan is a set of goals, interventions, and outcomes that guide the care of a client with a specific health problem, such as MI. The nurse should assess the client's level of anxiety and provide information and reassurance about his treatment plan.
Correct Answer is C
Explanation
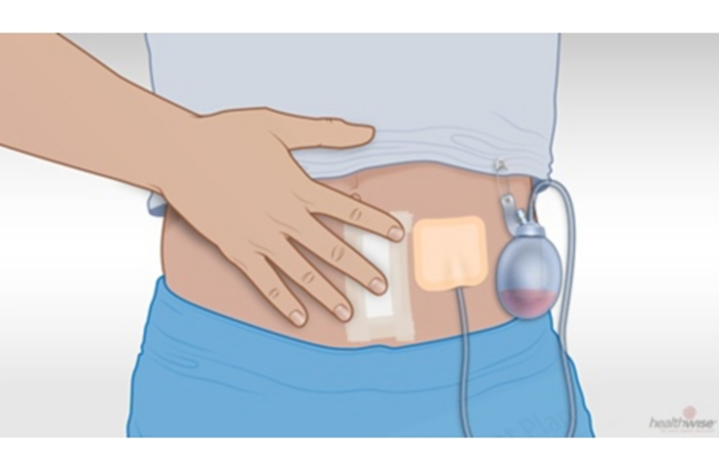
Choice C reason: observing the insertion site of a client who was discharged home with a suprapubic catheter can help detect signs of infection, bleeding, or healing problems. The nurse should inspect the incision site for redness, swelling, drainage, or odor and report any abnormal findings.
Choice A reason: measuring abdominal girth of a client who was discharged home with a suprapubic catheter is not necessary unless there are signs of urinary retention or obstruction. The nurse should monitor the urine output and color and report any changes.
Choice B reason: assessing perineal area of a client who was discharged home with a suprapubic catheter is not necessary unless there are signs of infection or irritation. The nurse should instruct the client on how to keep the perineal area clean and dry and report any discomfort or discharge.
Choice D reason: palpating flank area of a client who was discharged home with a suprapubic catheter is not necessary unless there are signs of urinary tract infection or kidney involvement. The nurse should ask the client about any pain or tenderness in the flank area and report any positive findings.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today