A client is receiving continuous ambulatory peritoneal dialysis since the arteriovenous (AV) graft in the right arm is no longer available for use for hemodialysis. The client has lost weight, has increasing peripheral edema, and has a serum albumin level of 1.5 g/dL (15 g/L). Which intervention is the priority for the nurse to implement?
Serum Albumin Reference Range: 3.5 to 5.5 g/dL (35 to 55 g/L)
Recommend the use of support stockings to enhance venous return
Ensure the client receives frequent small meals containing complete proteins
Evaluate patency of the AV graft for resumption of hemodialysis
Instruct the client to continue to follow the prescribed rigid fluid restriction amounts
The Correct Answer is B
Choice A reason: Support stockings may help with peripheral edema, but they are not the priority intervention for this client. The client's low serum albumin level indicates malnutrition and increased risk of infection and poor wound healing.
Choice B reason: This is the correct answer because the client needs adequate protein intake to maintain serum albumin levels and prevent further complications. Complete proteins contain all nine essential amino acids that the body cannot synthesize and are found in animal sources such as meat, eggs, and dairy products.
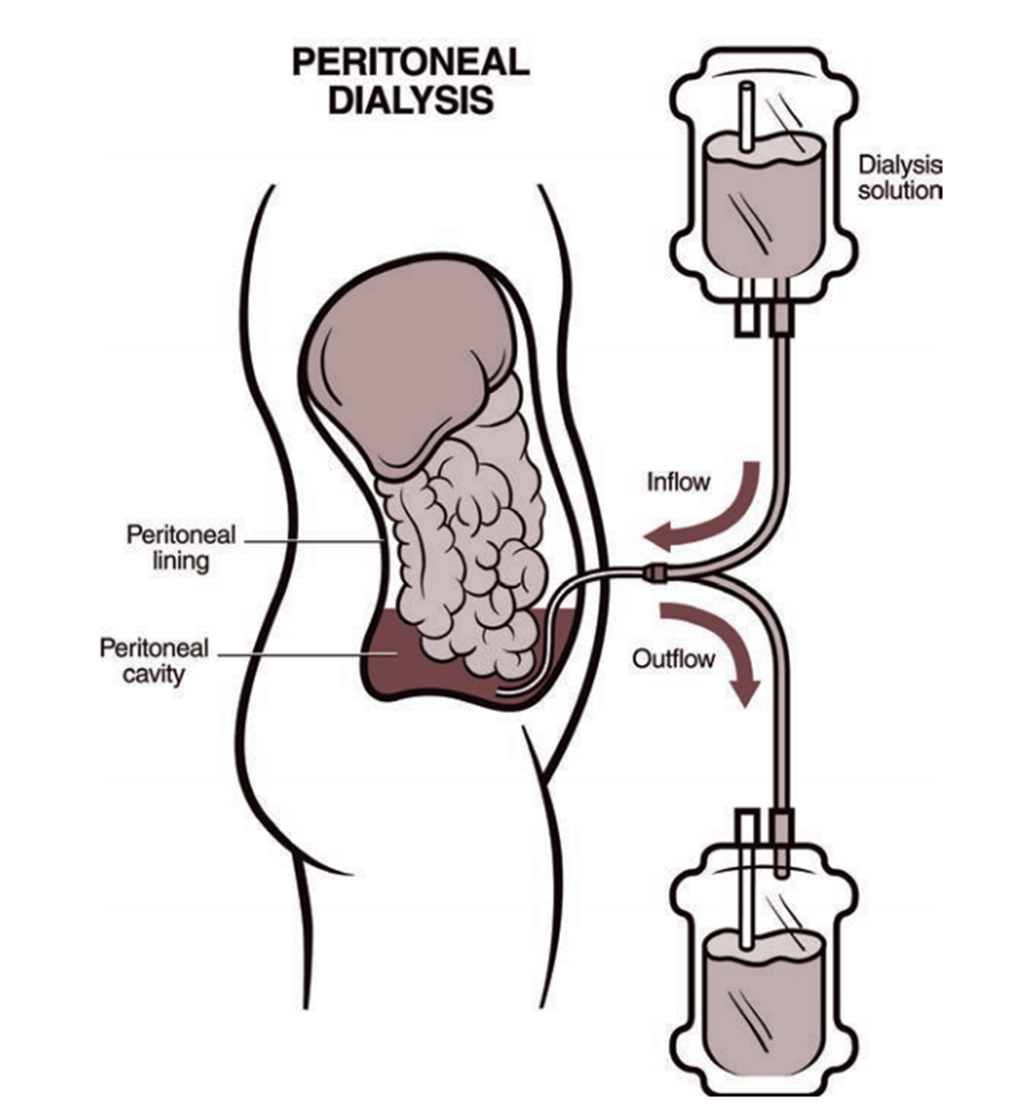
Choice C reason: Evaluating patency of the AV graft is not the priority intervention for this client because the client is receiving peritoneal dialysis, not hemodialysis. The AV graft may be used in the future if peritoneal dialysis fails, but it is not an immediate concern.
Choice D reason: Instructing the client to follow fluid restriction amounts is important for peritoneal dialysis patients, but it is not the priority intervention for this client. The client's low serum albumin level indicates that fluid restriction alone is not sufficient to manage fluid balance and prevent edema.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: Centering attention on positive upbeat music is not a specific instruction for the nurse to include, as this is a general coping strategy that may or may not be helpful for this client. This is a distractor choice.
Choice B reason: Finding outlets for more social interaction is not a relevant instruction for the nurse to include, as this may not address the underlying causes of anxiety or stress for this client. This is another distractor choice.
Choice C reason: Practicing using muscle relaxation techniques is an appropriate instruction for the nurse to include, as this can help reduce physical tension and promote calmness and relaxation for this client. Therefore, this is the correct choice.
Choice D reason: Thinking about reasons the episodes occur is not a helpful instruction for the nurse to include, as this can increase rumination and anxiety for this client. This is another distractor choice.
Correct Answer is D
Explanation
Choice A reason: Creatinine is not a relevant laboratory test for the nurse to monitor, as this reflects renal function and is not affected by naproxen or arthritis. This is a distractor choice.
Choice B reason: Serum calcium is not a pertinent laboratory test for the nurse to monitor, as this indicates bone metabolism and is not related to naproxen or arthritis. This is another distractor choice.
Choice C reason: Erythrocyte sedimentation rate is not an important laboratory test for the nurse to monitor, as this measures inflammation and is not influenced by naproxen or stomach pain. This is another distractor choice.
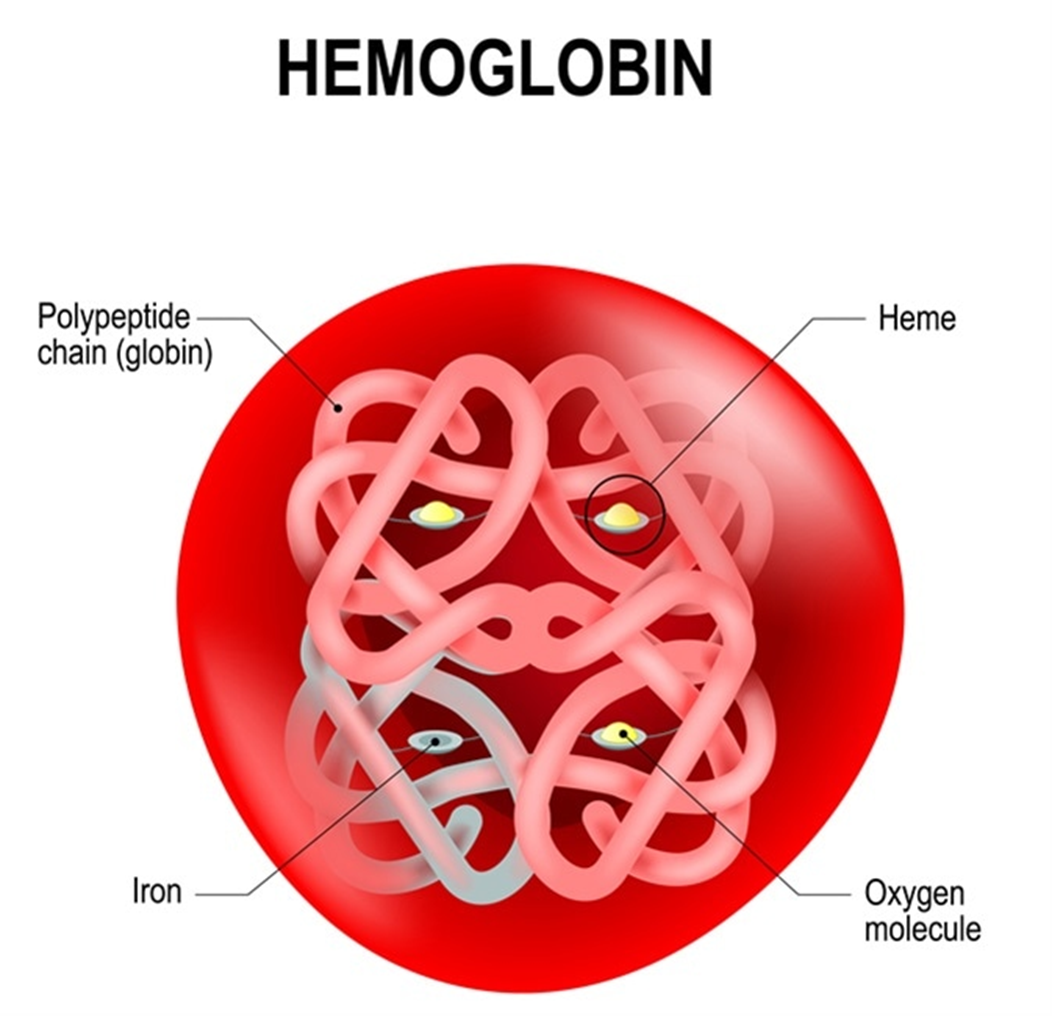
Choice D reason: Hemoglobin is an essential laboratory test for the nurse to monitor, as this shows blood oxygen-carrying capacity and can be reduced by naproxen-induced gastrointestinal bleeding, which can cause stomach pain, weakness, and fatigue. Therefore, this is the correct choice.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today