A nurse is caring for a 3-year-old child who was admitted with acute diarrhea and dehydration. Which of the following findings indicates that oral rehydration therapy has been effective?
Respiratory rate of 24 breaths/min
Heart rate of 130/min
Urine specific gravity of 1.015
Capillary refill of greater than 3 seconds
The Correct Answer is C
Choice A reason: A respiratory rate of 24 breaths/min is within the normal range for a 3-year-old child. It does not indicate the degree of hydration or dehydration of the child.
Choice B reason: A heart rate of 130/min is above the normal range for a 3-year-old child, which is 80 to 120/min. It may indicate dehydration, fever, pain, or anxiety. It does not indicate the effectiveness of oral rehydration therapy.
Choice C reason: A urine specific gravity of 1.015 is within the normal range for a child, which is 1.005 to 1.030. It indicates that the child's urine is adequately concentrated and that the child is well hydrated. It is a reliable indicator of the effectiveness of oral rehydration therapy.

Choice D reason: A capillary refill of greater than 3 seconds is abnormal and indicates poor peripheral perfusion. It may be a sign of dehydration, shock, or hypothermia. It does not indicate the effectiveness of oral rehydration therapy.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
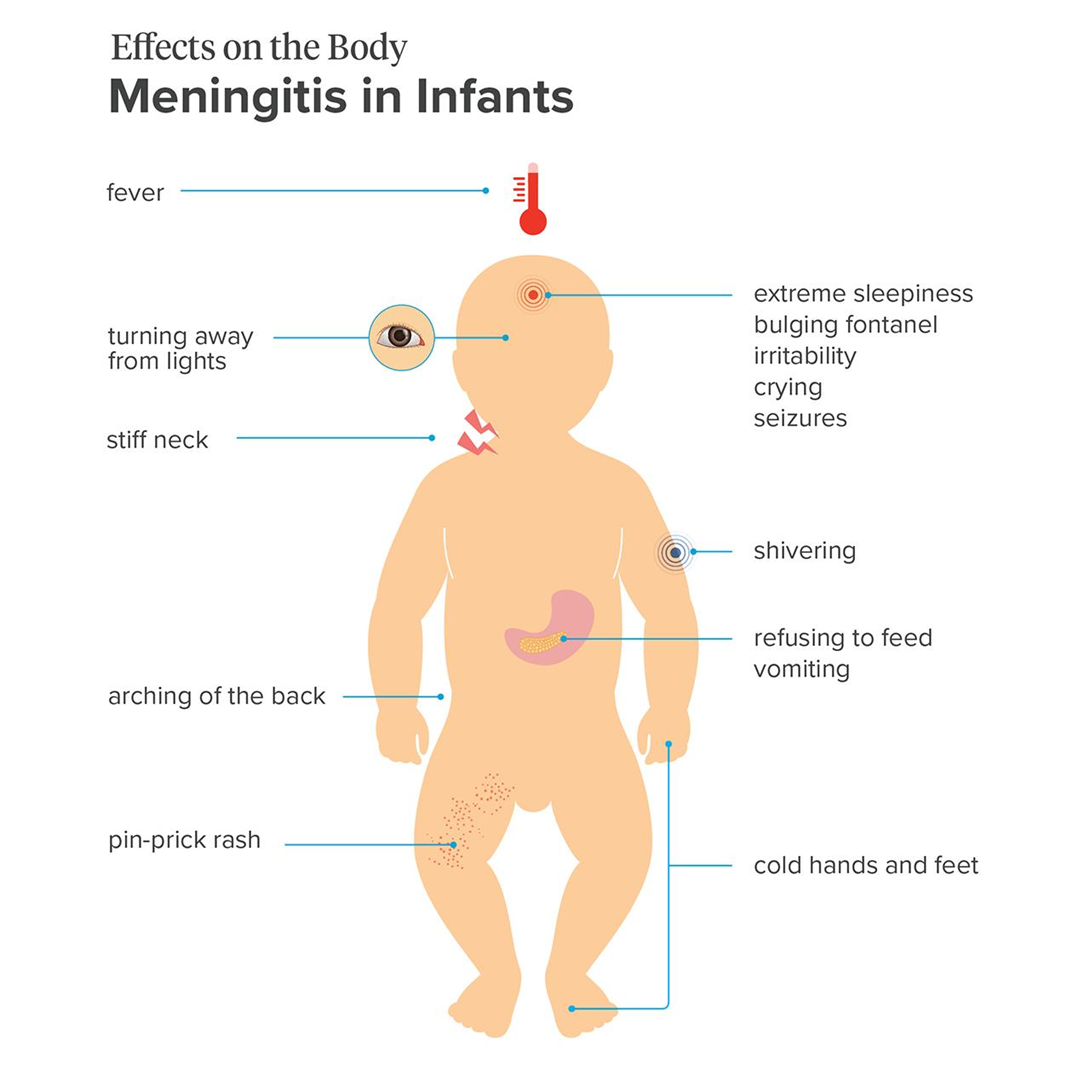
Choice A reason: Meningitis is a possible condition, as it is an inflammation of the membranes that cover the brain and spinal cord. It can be caused by various microorganisms, such as bacteria, viruses, or fungi. The infant has many signs and symptoms of meningitis, such as fever, irritability, lethargy, bulging fontanel, and clear cerebrospinal fluid from the lumbar puncture.
Choice B reason: Hydrocephalus is not a likely condition, as it is an accumulation of cerebrospinal fluid in the brain, which causes increased intracranial pressure and enlargement of the head. The infant has a bulging fontanel, which can indicate increased intracranial pressure, but not necessarily hydrocephalus. The infant does not have other signs of hydrocephalus, such as a rapidly increasing head circumference, prominent scalp veins, or sunset eyes.
Choice C reason: Intracranial hemorrhage is not a probable condition, as it is a bleeding within the skull, which can result from trauma, vascular malformation, or coagulation disorder. The infant has retinal hemorrhages, which can indicate intracranial hemorrhage, but not necessarily. The infant does not have other signs of intracranial hemorrhage, such as seizures, vomiting, or altered mental status.
Choice D reason: Sepsis is not a definite condition, as it is a systemic inflammatory response to an infection, which can cause organ dysfunction and shock. The infant has a fever, which can indicate sepsis, but not necessarily. The infant does not have other signs of sepsis, such as tachycardia, tachypnea, hypotension, or poor perfusion.
Correct Answer is ["A","B","C","D"]
Explanation
Choice A reason: This is a finding that the nurse should report to the provider. A pressure dressing is applied to the site of the catheter insertion to prevent bleeding and hematoma formation. If the dressing is saturated with bloody drainage, it indicates that the bleeding is not controlled and may lead to hemorrhage or infection.
Choice B reason: This is a finding that the nurse should report to the provider. Pulses of the extremity where the catheter was inserted should be equal to or stronger than the other extremity. If the pulses are diminished, it indicates that there is impaired blood flow to the extremity, which may be caused by arterial occlusion, thrombosis, or vasospasm.
Choice C reason: This is a finding that the nurse should report to the provider. The color and temperature of the extremity where the catheter was inserted should be similar to the other extremity. If the extremity is cool and pale, it indicates that there is inadequate perfusion to the extremity, which may be caused by the same factors as the diminished pulses.
Choice D reason: This is a finding that the nurse should report to the provider. Pain is an indicator of tissue damage or inflammation. The adolescent should have minimal or no pain after the procedure, as the site is numbed with local anesthesia. If the pain is present or increases, it indicates that there is a complication, such as bleeding, infection, or nerve injury.
Choice E reason: This is not a finding that the nurse should report to the provider. The apical pulse is the heart rate measured at the apex of the heart. It is a routine vital sign that the nurse should monitor after the procedure, but it is not a sign of a complication unless it is abnormal, such as too fast, too slow, or irregular. The nurse should compare the apical pulse with the baseline and the expected range for the adolescent's age and condition.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today