An older adult male client arrives at the clinic reporting that his bladder always feels full. The client also reports a weak urine flow, frequent dribbling after voiding, and increasing nocturia with difficulty initiating the urine stream. Which action should the nurse implement?
Obtain a urine specimen for culture and sensitivity.
Instruct in effective techniques to cleanse the glans penis.
Palpate the client's suprapubic area for distention.
Advise the client to maintain a voiding diary for one week.
The Correct Answer is C
Choice A reason: While obtaining a urine specimen is important for diagnosing infection, it does not address the immediate discomfort and potential urinary retention the client may be experiencing.
Choice B reason: Cleansing the glans penis is part of good hygiene but does not address the client's symptoms of a full bladder and weak urine flow.
Choice C reason: Palpating for suprapubic distention can provide immediate information about bladder fullness and potential urinary retention, which may require prompt intervention.
Choice D reason: Maintaining a voiding diary is useful for tracking symptoms over time but does not provide an immediate assessment or intervention for the client's current symptoms.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice A reason: Application of heat and cold therapy can help manage symptoms but does not encompass the broader aspects of health promotion and teaching.
Choice B reason: Avoidance of foods containing purine is more specific to conditions like gout rather than rheumatoid arthritis, and while diet is important, it does not fully represent health promotion and teaching.
Choice C reason: Immobilization of affected joints is not a health promotion strategy and can actually worsen symptoms over time. Active and passive range-of-motion exercises are recommended instead.
Choice D reason: Prevention through nutrition and exercise is the most comprehensive approach that aligns with health promotion and teaching for clients with rheumatoid arthritis. It includes educating clients on a balanced diet and physical activity to manage symptoms and improve overall health.
Correct Answer is C
Explanation
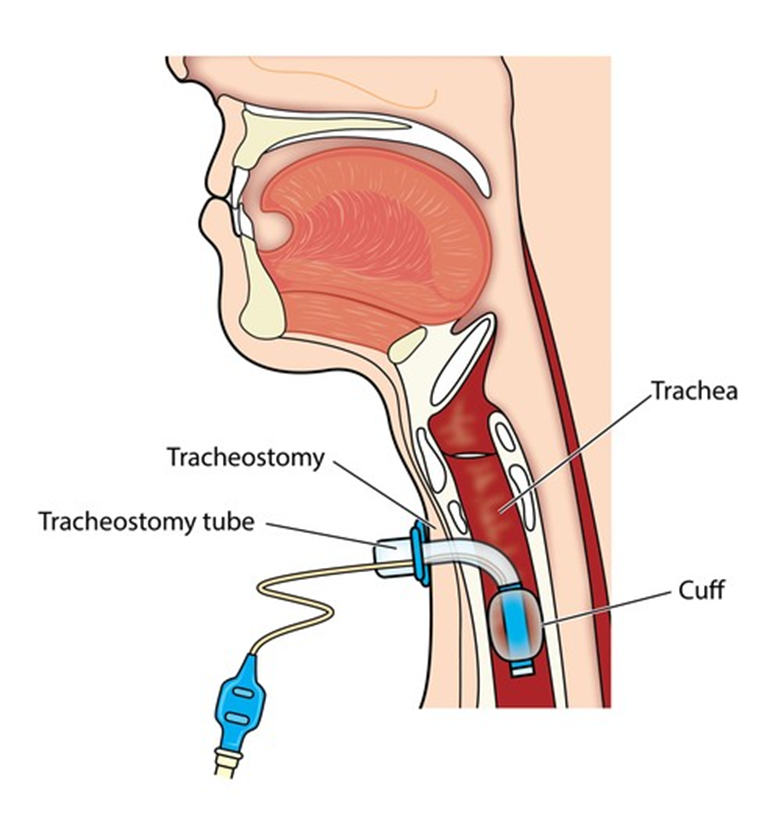
Choice A reason: Applying a water-soluble lubricant to the catheter is not recommended during tracheostomy suctioning as it may introduce contaminants.
Choice B reason: Instilling sodium chloride before suctioning is not a standard practice and can lead to complications such as edema.
Choice C reason: Wearing protective goggles is important to protect the nurse from potential splashes of bodily fluids during the suctioning process.
Choice D reason: Instructing the client to cough as the suction tip is removed is not recommended as it can cause discomfort and potential harm to the tracheal lining.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today