After initiating a steroid nebulizer treatment for a client with asthma in respiratory distress, which intervention is most important for the nurse to implement?
Monitor pulse oximetry every 2 hours.
Teach proper use of a rescue inhaler.
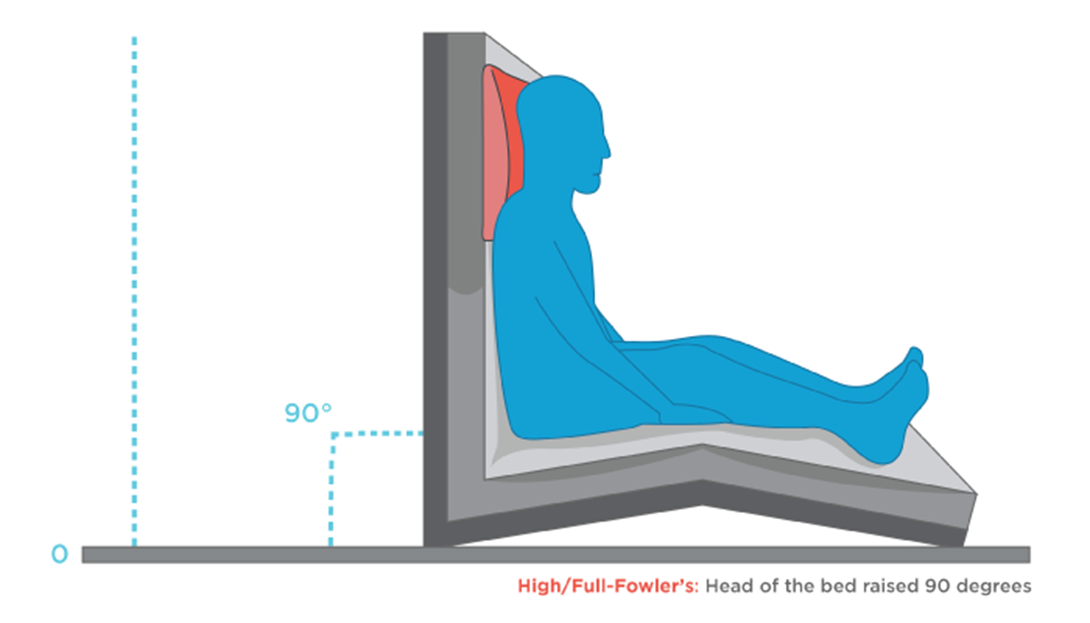
Elevate the head of bed to 90 degrees.
Determine exposure to asthmatic triggers.
The Correct Answer is C
Choice A reason: This is incorrect because monitoring pulse oximetry every 2 hours is not a sufficient or timely intervention for the nurse to implement. Pulse oximetry is a noninvasive method of measuring the oxygen saturation of hemoglobin in the blood. Normal oxygen saturation is 95% to 100%, while hypoxemia is less than 90%. However, pulse oximetry may not reflect the severity of respiratory distress or the effectiveness of nebulizer treatment in a client with asthma. Moreover, monitoring pulse oximetry every 2 hours is too infrequent for a client who is in acute respiratory distress and needs more frequent assessment and intervention.
Choice B reason: This is incorrect because teaching proper use of a rescue inhaler is not a priority or relevant intervention for the nurse to implement. A rescue inhaler is a type of short-acting bronchodilator that can be used to relieve acute asthma symptoms by relaxing the smooth muscles of the airways and improving airflow. However, teaching proper use of a rescue inhaler is not an urgent action for a client who is already receiving nebulizer treatment, which delivers a higher dose of medication directly to the lungs. Moreover, teaching proper use of a rescue inhaler is not appropriate for a client who is in respiratory distress and may not be able to focus or retain information.
Choice C reason: This is correct because elevating the head of bed to 90 degrees is the most important intervention for the nurse to implement. Elevating the head of bed to 90 degrees can help improve breathing and oxygenation by reducing pressure on the diaphragm and chest wall, increasing lung expansion and ventilation, and facilitating expectoration of mucus. This can enhance the effects of nebulizer treatment and reduce respiratory distress in a client with asthma.
Choice D reason: This is incorrect because determining exposure to asthmatic triggers is not an immediate or helpful intervention for the nurse to implement. Asthmatic triggers are substances or factors that can cause or worsen asthma symptoms by inducing inflammation or constriction of the airways. Examples of asthmatic triggers include allergens, irritants, infections, exercise, stress, or weather changes. However, determining exposure to asthmatic triggers is not a priority action for a client who is in respiratory distress and needs more urgent interventions to improve breathing and oxygenation. Moreover, determining exposure to asthmatic triggers may not change the management or outcome of an acute asthma attack that has already occurred.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: Irregular ulcer shapes and severe edema are characteristic of venous ulcers, which are caused by impaired venous return and increased capillary pressure. Venous ulcers are usually located near the medial malleolus and have a shallow depth.
Choice B reason: Hairless lower extremities and cool feet are signs of arterial insufficiency, which reduces blood flow and oxygen delivery to the tissues. Arterial ulcers are usually located on the toes, heels, or lateral malleoli and have a deep, punched-out appearance.
Choice C reason: Black ulcers and dependent rubor are also signs of arterial insufficiency, indicating tissue necrosis and inflammation. Dependent rubor is a reddish-blue color of the lower extremity that occurs when the leg is lowered below the level of the heart.
Choice D reason: Absent pedal pulses and shiny skin are also signs of arterial insufficiency, indicating reduced blood flow and atrophy of the skin. The skin may also be dry, scaly, or cracked.
Correct Answer is {"dropdown-group-1":"A","dropdown-group-2":"C","dropdown-group-3":"D","dropdown-group-4":"A"}
Explanation
The client has inhaled smoke, which can cause respiratory problemssuch as airway obstruction, bronchospasm, and pulmonary edema. The client also has initial fluid shifts, which can lead to electrolyte imbalancesuch as hyponatremia, hyperkalemia, and metabolic acidosis.
Choice A: inhaled smoke - respiratory problems
This is a correct choice. Inhaled smoke can damage the respiratory system by causing inflammation, edema, and carbon monoxide poisoning.
Choice B: initial fluid shifts - electrolyte imbalance
This is a correct choice. Initial fluid shifts occur when fluid moves from the intravascular space to the interstitial space due to increased capillary permeability. This can result in electrolyte imbalance such as low sodium, high potassium, and low bicarbonate levels.
Choice C: increased cardiac output - high blood sodium levels
This is an incorrect choice. Increased cardiac output is not a condition that occurs in burn patients. High blood sodium levels are not a common finding in burn patients either. High blood sodium levels can occur due to dehydration or excessive sodium intake.
Choice D: decreased catecholamines - hypometabolism
This is an incorrect choice. Decreased catecholamines are not a finding in burn patients. Catecholamines are hormones that increase heart rate, blood pressure, and metabolism in response to stress. Burn patients have increased catecholamines due to pain and tissue injury. Hypometabolism is also not a condition that occurs in burn patients. Hypometabolism is a state of low metabolic rate that can occur due to starvation, hypothyroidism, or hypothermia. Burn patients have increased metabolism due to increased energy demands for wound healing and thermoregulation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today