Exhibits
Specify which potential condition the client is most likely experiencing, two actions the nurse should take to address that condition, and two parameters the nurse should monitor to assess the client’s response.
The Correct Answer is []
- The client is most likely experiencing compartment syndrome, which is a condition where increased pressure within a closed space compromises blood flow and tissue perfusion. Compartment syndrome can occur after a fracture, especially if a cast or splint is applied too tightly. Some of the signs and symptoms of compartment syndrome are severe pain, paresthesia, pallor, and pulselessness.
- Two actions the nurse should take to address compartment syndrome are:
- Elevate the extremity above the level of the heart to reduce swelling and improve venous return.
- Remove the cast or loosen the dressing to relieve the pressure and restore blood flow. This may require notifying the physician or obtaining an order for bivalving or cutting the cast.
- Two parameters the nurse should monitor to assess the client’s condition are:
- Capillary refill of the affected fingers, which should be less than 3 seconds. A prolonged capillary refill indicates poor perfusion and tissue ischemia.
- Blood pressure of the client, which should be maintained within normal limits. Hypotension can worsen the perfusion deficit and lead to tissue necrosis.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
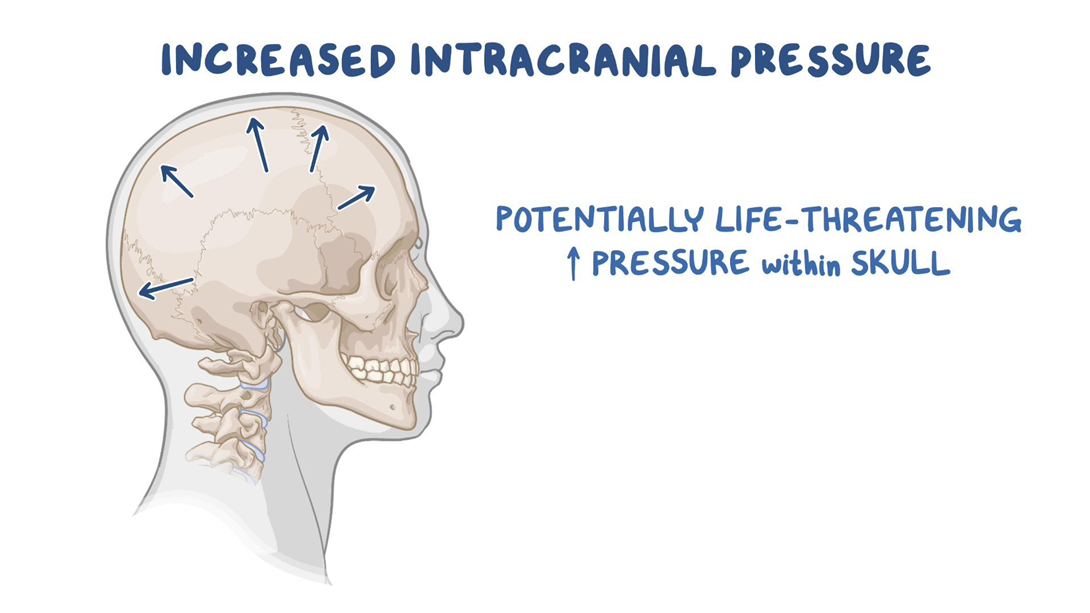
Choice A reason: Pupillary changes to ipsilateral dilation indicate increased intracranial pressure, which is a life-threatening complication of stroke. The nurse should notify the physician and prepare for emergency measures.
Choice B reason: Left-sided facial drooping and dysphagia are common signs of right hemisphere stroke, but they do not require immediate intervention by the nurse. The nurse should monitor the patient's swallowing ability and provide oral care.
Choice C reason: Orientation to person and place only is a sign of impaired cognition, which is also common in right hemisphere stroke. The nurse should assess the patient's memory, judgment, and attention span.
Choice D reason: Unequal bilateral hand grip strengths are a sign of hemiparesis, which is a weakness on one side of the body. The nurse should assist the patient with mobility and prevent contractures.
Correct Answer is C
Explanation
Choice A reason: Lifting and clearing drainage from the chest tube is not necessary, as the water level fluctuations indicate that the chest tube is functioning properly and allowing air and fluid to escape from the pleural space.
Choice B reason: Inspecting the tube insertion site for leaking is not indicated, as there is no evidence of air leak in the water-seal chamber. An air leak would cause continuous or intermittent bubbling in the water-seal chamber.
Choice C reason: Continuing to monitor the drainage system is the best action for the nurse to implement, as the water level fluctuations are normal and expected in a water-seal drainage system. The water level should rise during inspiration and fall during expiration, reflecting the changes in intrathoracic pressure.
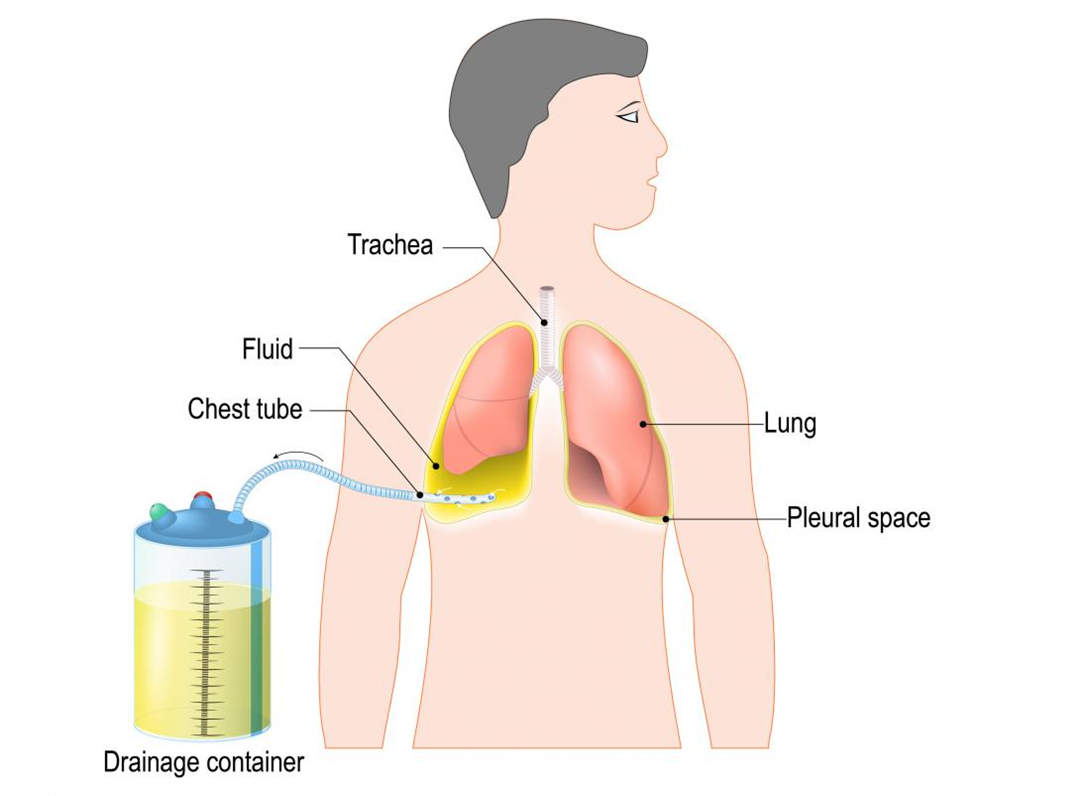
Choice D reason: Auscultating lungs for unequal breath sounds is not relevant, as it does not address the question of what to do with the water level fluctuations. Unequal breath sounds may indicate a pneumothorax or atelectasis, which are complications of chest trauma or chest tube insertion.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today